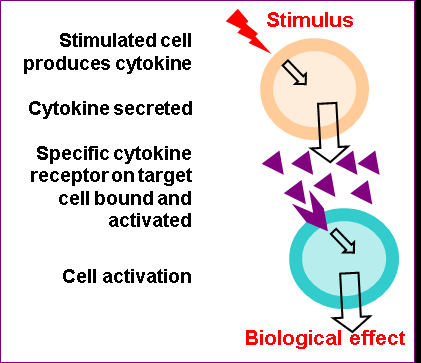
Cytokines are soluble protiens/polypeptides, produces by a variety of hematopoetic and non hematopoetic cell types. They are responsible for the regulation of immunological, inflammatory and reparative host responses.
Cytokines tend to bind to high affinity receptors and the target cells and mediate their effects. Specific cytokines mediate specific reactions.
Reference: Arvind Arora
Cytokines basically mediate immune response. But some cytokines are also pro inflammatory.
These are:-
Il-1, TNF alpha and IL-6.
IL-1 is the most important pro inflammatory cytokine.
Anti inflammatory cytokines are involved in the resolution of inflammation. These include:
IL-4, IL-10 IL-13 and TGF beta.
IL-4 has mainly anti-inflammatory properties with some pro-inflammatory properties.
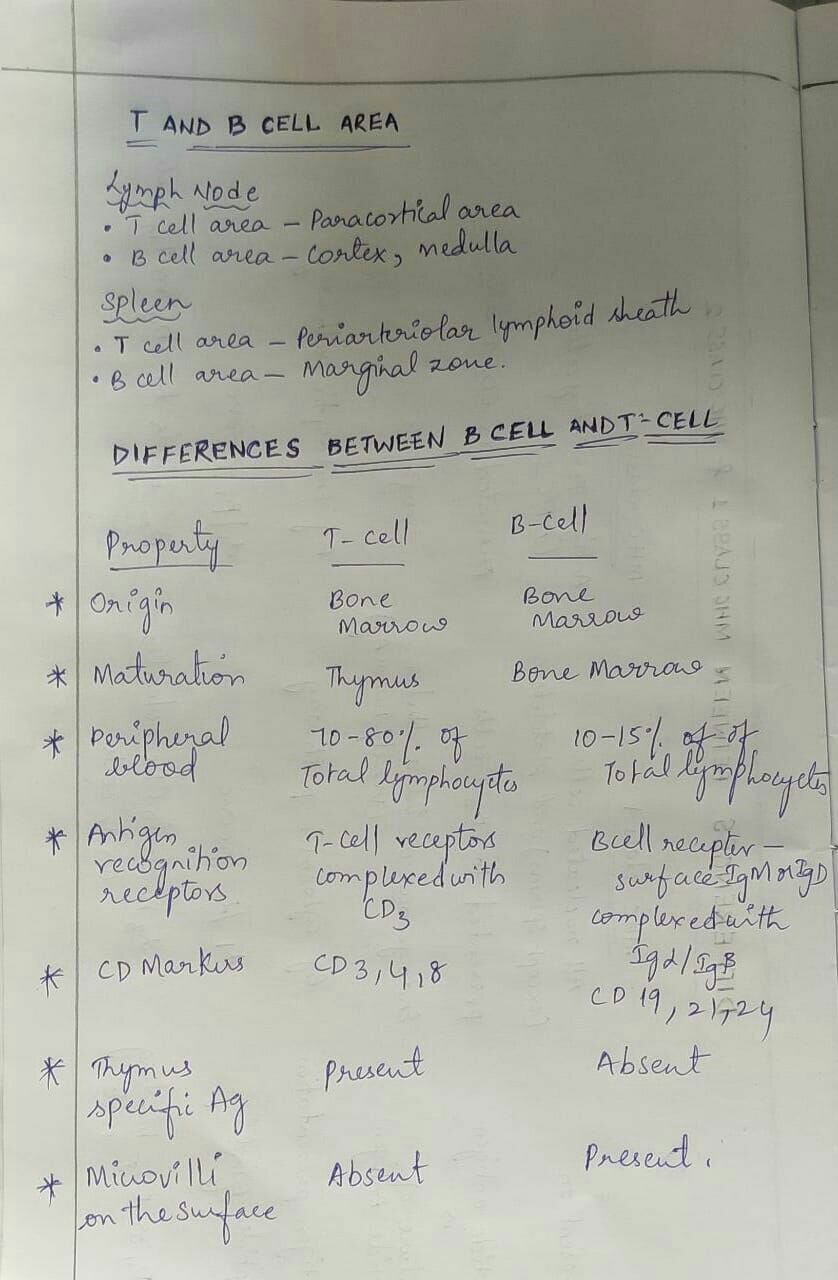
T- cells are among the two important cells of the adaptive immune system (others are B- Cells). T-cells arise in the bone marrow and mature in the thymus.
T- cells constitute 60-70% of the circulating peripheral lymphocytes.
T- cells categories:-
1.) Helper or Inducer T-cells:
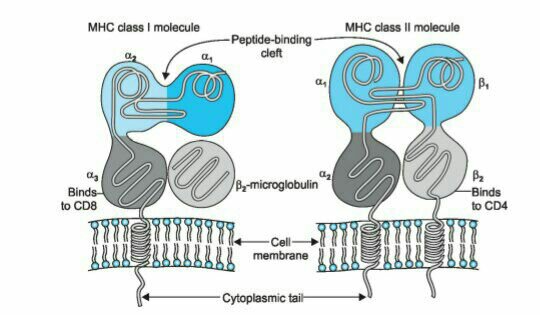
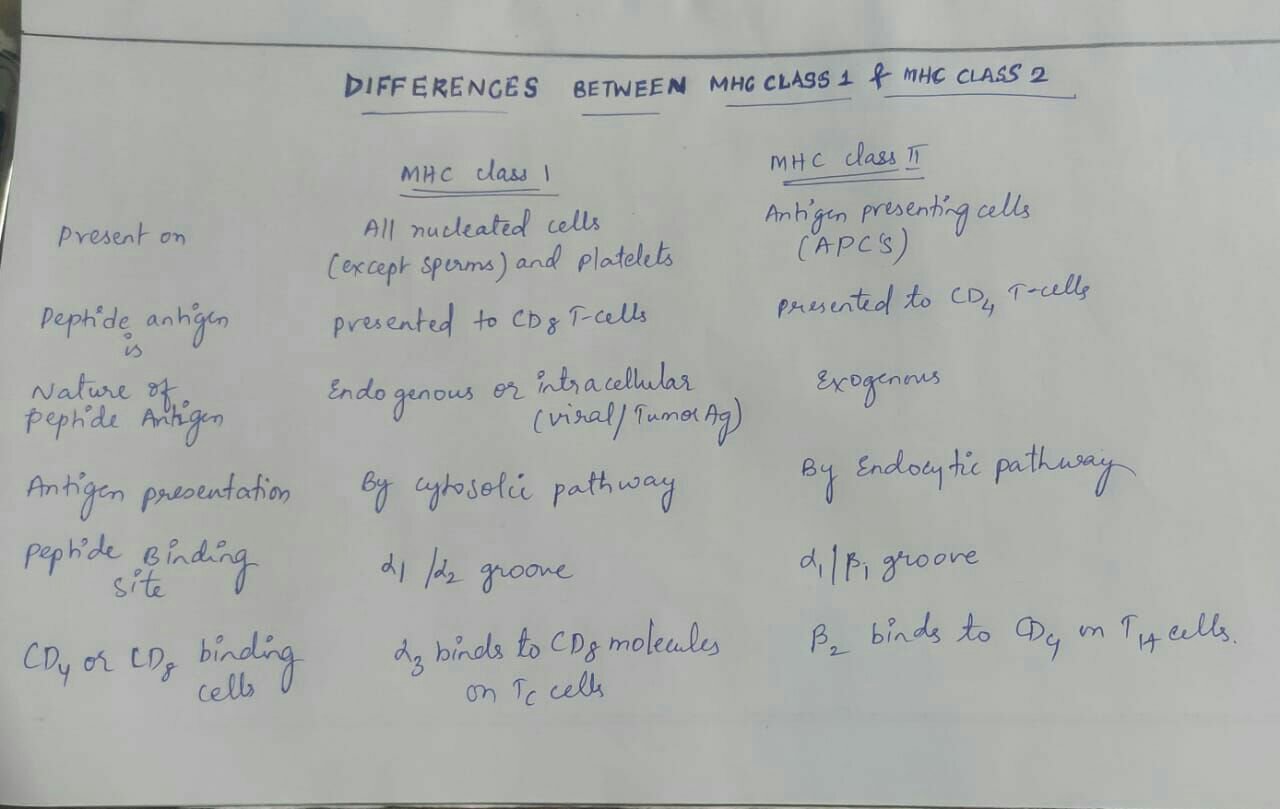
60% of T- cells are helper T- cells. They have CD4 surface marker and are MHC II restricted. Types of CD4 helper cells are:
A) Effector cells- TH1, TH2 and TH17 cells. The TH1 cells are activated by IFN- gamma and themselves produce IL-2, IFN-gamma and IL-12. They are the primary cells involved in delayed hypersensitivity, cell mediated immunity, macrophage activation and killing of intracellular microbes. TH2 cells are activated by IL4 and themselves produce IL4, IL5, IL6 and IL13. They produce all antibodies except for IgG2b and also provide defence against helminthic parasites. TH17 cells are powerful recruiters of neutrophils and monocytes to play a role in severe inflammatory diseases.
B) Memory cells- They retain the antigenic affinity of previously activated T-cells and are used in a second immune response.
2.) Cytotoxic T-cells:
30% of the total T-cells. They have CD8 surface marker and MHC I restricted. They kill amd lyse target cells which include tumour cells, virus infected cells and allograft.
THE RATIO OF CD4:CD8 T-cell is normally 2:1.
3.) Suppressor T-cells:
They have CD8 surface marker and are MHC I restricted. They are responsible for down regulation of the immune response.
T–CELL RECEPTOR (TCR)
TCR is a molecule found on the T-cell which is responsible for recognising the antigen bound to MHC molecule. It is a heterodomer made up of an alpha and a beta chain. The presence of TCR gene rearrangements demonstrated by molecular analysis is a marker of T-cell lineage.
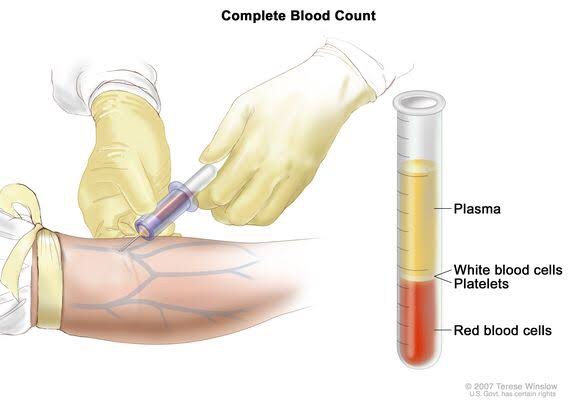
A blood sample drawn from a vein in your arm or a fingerstick or heelstick (newborns)
• Test Preparation Needed?
None
• Why get tested?
To determine your general health status; to screen for, diagnose or monitor any one of a variety of diseases and conditions that affect blood cells, such as anemia, infection, inflammation, bleeding disorder or cancer.
• Also known as: Hgb; Hb; H and H (Hemoglobin and Hematocrit)
• Sample Required?
A blood sample drawn from a vein in your arm or a fingerstick or heelstick (newborns)
• Test Preparation Needed?
None
• Why get tested?
To evaluate the hemoglobin content of your blood as part of a general health check-up; to screen for and help diagnose conditions that affect red blood cells (RBCs); If you have anemia (low hemoglobin) or polycythemia (high hemoglobin), to assess the severity of these conditions and to monitor response to treatment
• When to get tested?
With a hematocrit or as part of a complete blood count (CBC), which may be ordered as a component of a general health screen; when you have signs and symptoms of anemia (weakness, fatique) or polycythemia (dizziness, headache); at regular intervals to monitor these conditions or response to treatment
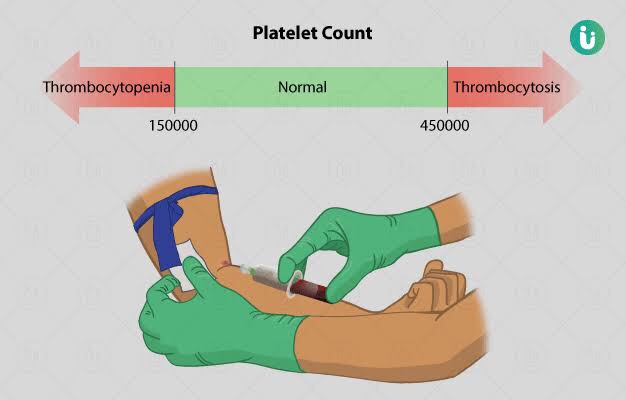
• Also known as: Thrombocyte count; PLT; Platelet distribution width; PDW; Mean Platelet volume; MPV.
• Sample Required?
A blood sample drawn from a vein in your arm or a fingerstick or heelstick (newborns)
• Test Preparation Needed?
None
• Why get tested?
To determine the number of platelets in a sample of your blood as part of a health exam; to screen for, diagnose, or monitor conditions that affect the number of platelets, such as a bleeding disorder, a bone marrow disease, or other underlying condition.
• When to get tested?
As part of a routine complete blood count (CBC); when you have episodes of unexplained or prolonged bleeding or other symptoms that may be due to a platelet disorder
• What is being tested?
Platelets, also called thrombocytes, are tiny fragments of cells that are essential for normal blood clotting. They are formed from very large cells called megakaryocytes in the bone marrow and are released into the blood to circulate. The platelet count is a test that determines the number of platelets in a person’s sample of blood. When there is an injury to a blood vessel or tissue and bleeding begins, platelets help stop bleeding.
• Also known as: Leukocyte differential count; Peripheral differential; WBC count differential; Diff; blood differential; Differential Blood Count
• Formal name: White blood cell differential
• Why get tested?
To help determine the cause of abnormal results on a WBC count; to help diagnose or monitor an illness affecting your immune system, such as an infection or inflammatory condition, or cancers that affect your white blood cells, such as leukemia.
• When to get tested?
As part of a CBC; when you have a routine health examination; when results of a CBC fall outside the reference range; when you have any number of signs and symptoms that may be related to a condition affecting white blood cells, such as infection, inflammation, or cancer, when you are receiving treatment that is known to affect WBCs, such as chemotherapy.
• What is being tested?
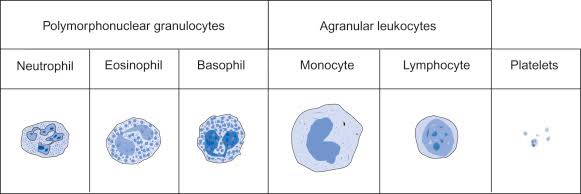
WBCs, also called leukocytes, are cells that circulate in the blood and the lymphatic system that help protect the body against infections. They are an important part of the body’s immune system and also have a role in inflammation, allergic responses, and protection against cancer. A WBC differential totals the number of each of the different types of WBCs in a person’s sample of blood.
There are five types of white blood cells, each with different functions.
Red blood cells, also known as erythrocytes, make up thecellular part of blood, giving it its red color and also the ability to bind and carry oxygen to all parts of the body. Under a microscope, they appear to be circular and biconcave in shape.
Gives us the number of erythrocytes per cubic mm in circulating blood & Hb in blood.
Procedure done by office or chairside method and also automated procedure.
Hematological diseases of RBCs are anemia & polycythemia.
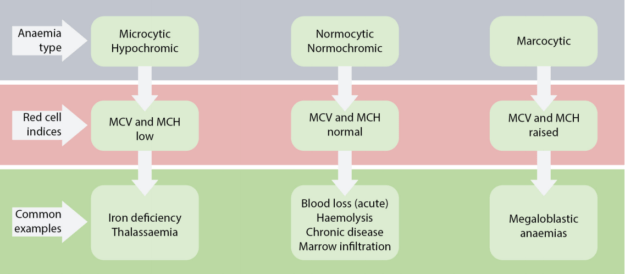
Categorized by mean corpuscular volume, anemia can be differentiated into microcytic, macrocytic and normocytic anemias. Normocytic anemia can be further divided into intrinsic and extrinsic RBC defect and blood loss.
MCV – Mean corpuscular volume is the average volume of red blood cells and is reflective of RBC size. When RBCs increase or decrease in size, the mean corpuscular volume changes; this helps physicians determine the type of anemia and its causes. Normal MCV is 80–96 µm³.
MCH stands for “mean corpuscular hemoglobin.” An MCH value refers to the average quantity of hemoglobin present in a single red blood cell.
MCHC is short for mean corpuscular hemoglobin concentration. MCHC refers to the average amount of hemoglobin inside a single red blood cell.
Hematocrit is the measure of the total volume % of red blood cells in the blood. The normal value for hematocrit is 45% for men and 40% for women. It is an important component of a patient’s complete blood profile.
• In microbiology we often come across this word typing in simplest words means classification of microorganisms
• Typing is broadly classified as
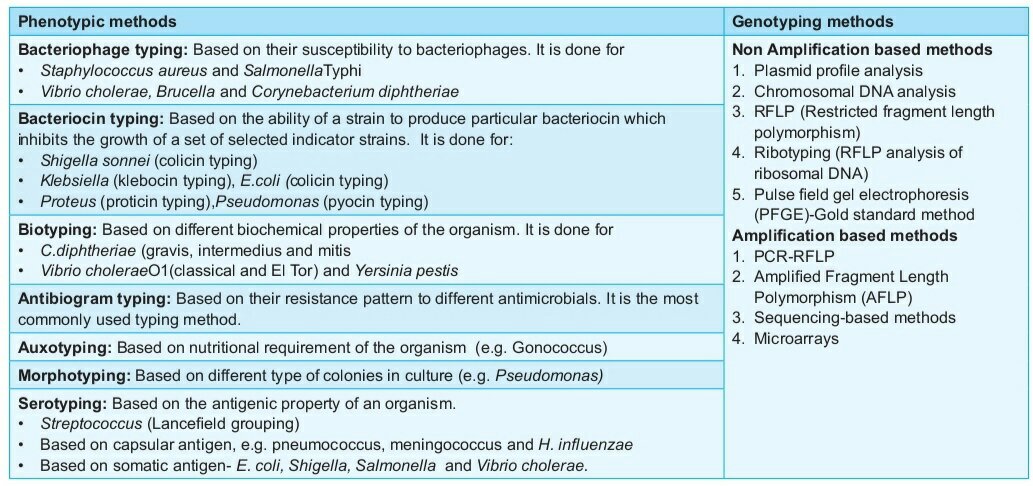
– Phenotypic methods
– Genotypic methods
• Genotypic methods are the ones which analyse the kind of genes present on chromosomes and plasmids of microorganisms. They are used to know whether the genes are homologous or heterologous
• And also to know certain specific genes whether they are present or absent and similar other attributes of the genes . They are way more complicated to do and interpret the results as these are expensive methods , hence they are not used in routine diagnostic purpose.
• phenotypic methods are the commonly used methods. These methods are used for diagnostic purpose. These methods are based on observable characters or physical characters of microorganism like shape, size, results from biochemical reaction, susceptibility or resistance to antibiotics or other certain viruses.
• Common type of phenotypic methods is serotyping. Serotyping refers to sero means surface and typing means classification. Serotyping is based on differences in the different structures decorated on the surface of microorganism.
• Serotyping is based on the surface structures such as lipopolysaccharides,membrane proteins, capsular polysaccharide, fimbriae and flagella.
➡️ Bacteriostatic antibiotics limit the growth of bacteria by interfering with bacterial protein production, DNA replication or other aspects of bacterial cellular metabolism.
They must work together with immune system to remove the micro-organisms from the body. Example:
Tetracyclins
Sulphonamides
Macrolides
Lincosamides
Chloramphenicol
trimethoprim
Most antimicrobial agents in clinical use are bactericidal,
Note that while it is rational to favor bactericidal agents over bacteriostatic agents, neither has ever been shown to be superior (probably because true recovery from infection cannot occur until the body is able to mount an appropriate immune response, thus “buying time” may be just as good as active killing)
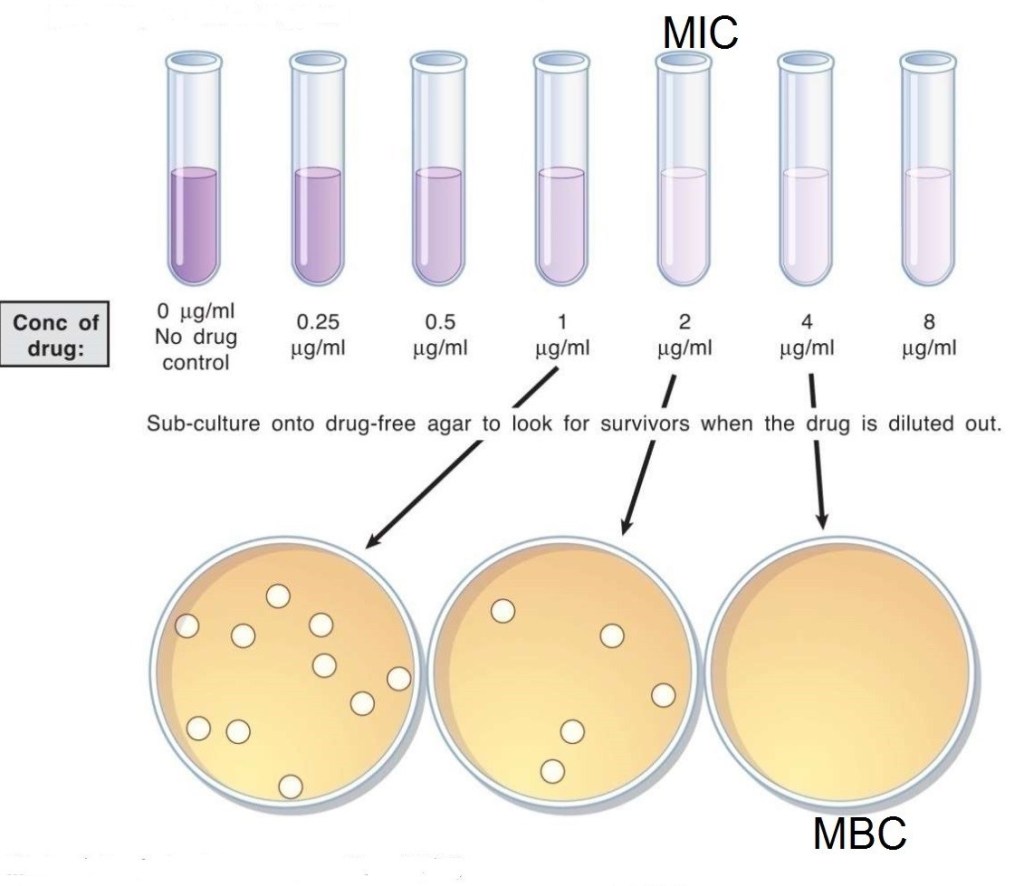
Minimum inhibitory concentration (MIC) versus minimum bactericidal concentration (MBC).
➡️ The MBC is the minimum concentration of drug which can kill the micro-organisms.
➡️ The MIC is the minimum concentration of drug which can inhibit the growth of micro-organisms.
🔷 CHOOSING APPROPRIATE ANTIBIOTIC (A Clinician’s guide to the CARAT criteria)
Council for Appropriate and Rational Antibiotic Therapy (CARAT) criteria for accurate use of antibiotic therapy ● Evidence-based results ●Therapeutic benefits ● Safety ● Cost-effectiveness ● Optimal drug dose and duration —Shorter-course, more aggressive therapy
(i) Evidence-based results:
In choosing an antibiotic, clinicians should consider the clinical evidence demonstrating that the drug is clinically and microbiologically appropriate, the efficacy of that drug in well-designed clinical trials, and the antibiotic resistance patterns of the local region. Clinicians should then use their professional judgment to choose the optimal antibiotic.
(ii) Therapeutic benefits:
If possible, the clinician should identify the causative pathogen and use surveillance data on regional antibiotic resistance patterns in selecting the optimal therapeutic agent.
(iii) Safety:
In treating patients with a particular drug, safety must be weighed against efficacy. Clinically applicable treatment strategies should be chosen to maximize efficacy while minimizing side effects.
(iv) Optimal drug for optimal duration:
Optimal drug selection requires finding the antimicrobial class and the specific member of that class that is best suited to treat a particular infection. Because empiric therapy is necessary in most cases, multiple factors have to be considered. Among these are whether the etiologic agent is likely to be gram-positive or gram-negative, whether a narrow or broad-spectrum agent should be chosen, the resistance patterns of the likely pathogen to this drug, both nationally and regionally, and the individual patient’s medical history, including recent antibiotic exposure.
Optimal duration means prescribing the selected drug for the shortest amount of time required for clinical and micro- biologic efficacy. There are many reasons for reducing an- timicrobial therapy to the shortest appropriate duration. They include the potential for reduced occurrence of adverse effects, increased patient adherence, decreased promotion of resistance, and decreased costs.
(v) Cost-effectiveness:
Choosing inappropriate therapy is associated with increased costs, including the cost of the antibiotic and increases in overall costs of medical care because of treatment failures and adverse events.