

Sources – Shafer’s textbook of oral pathology , Slideshare.com
Category: Hematology
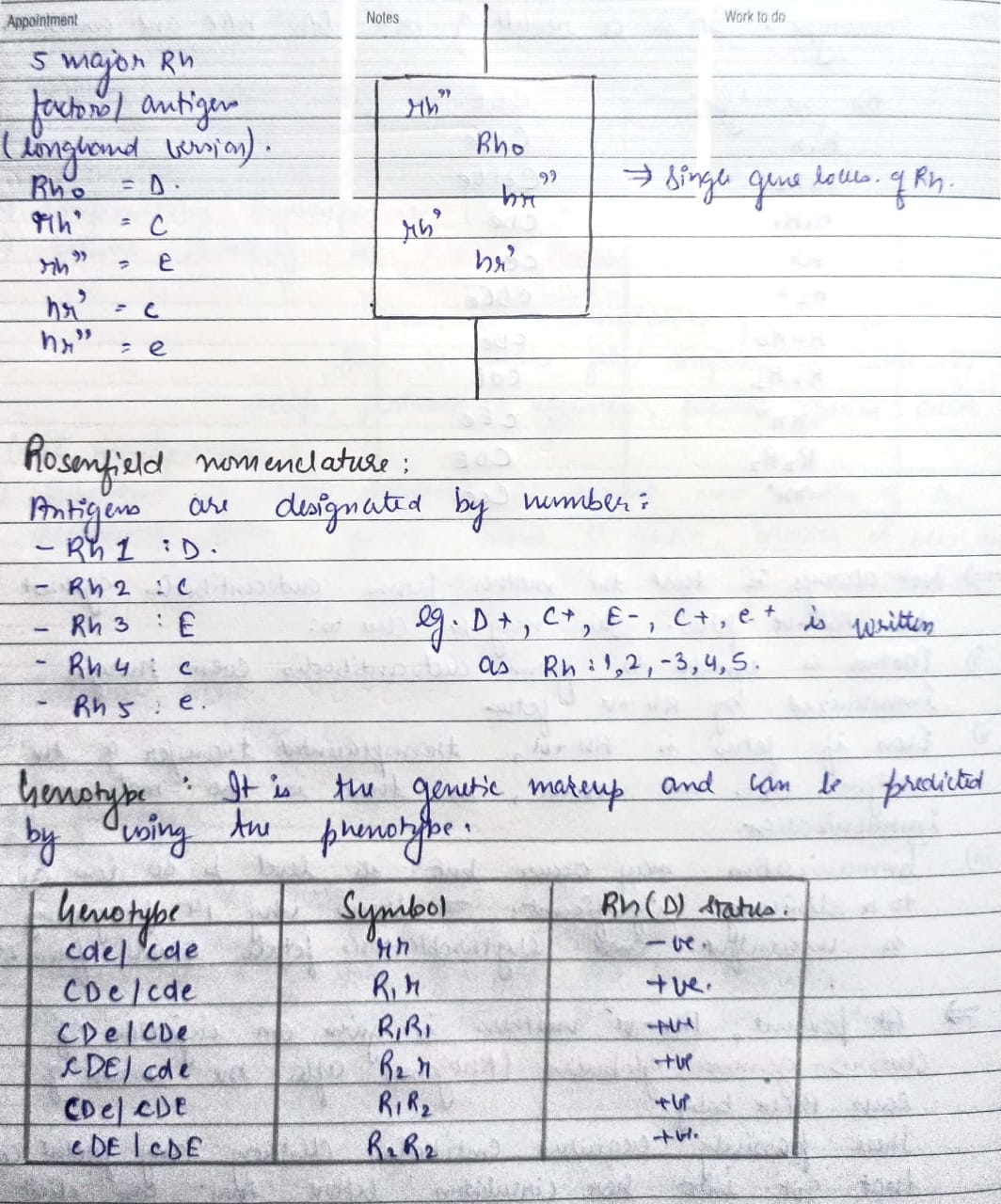
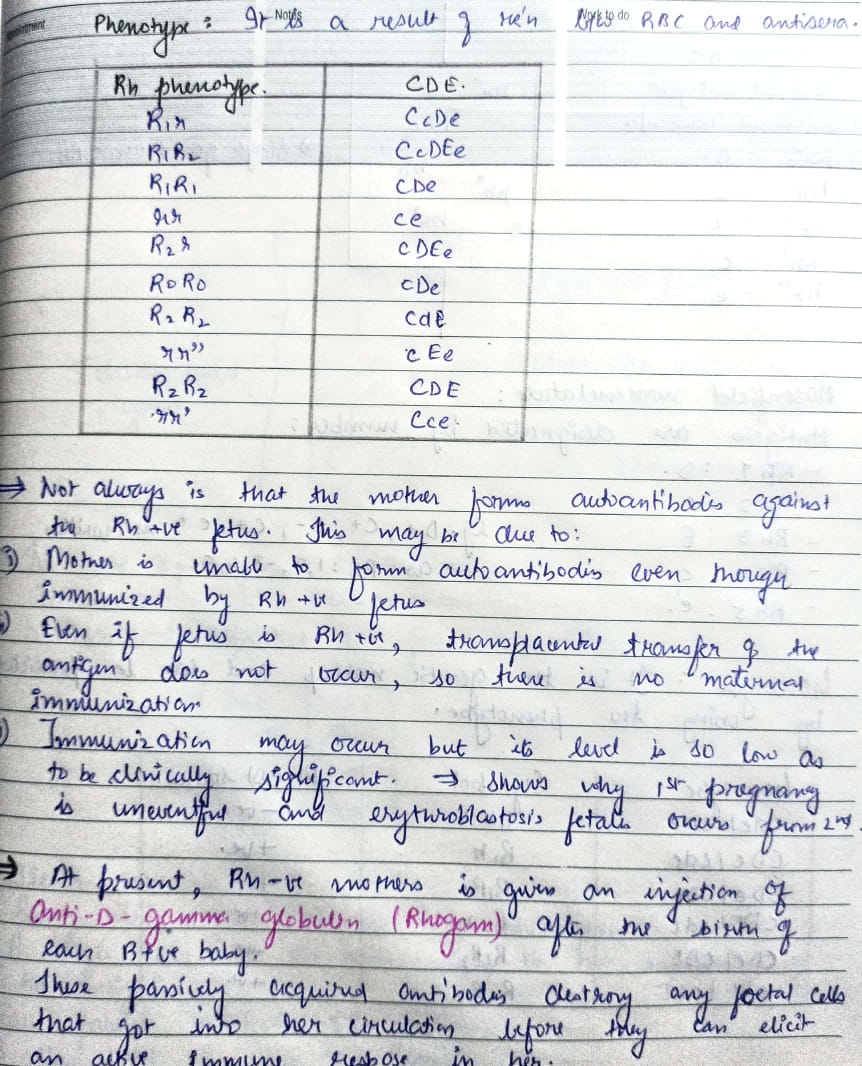
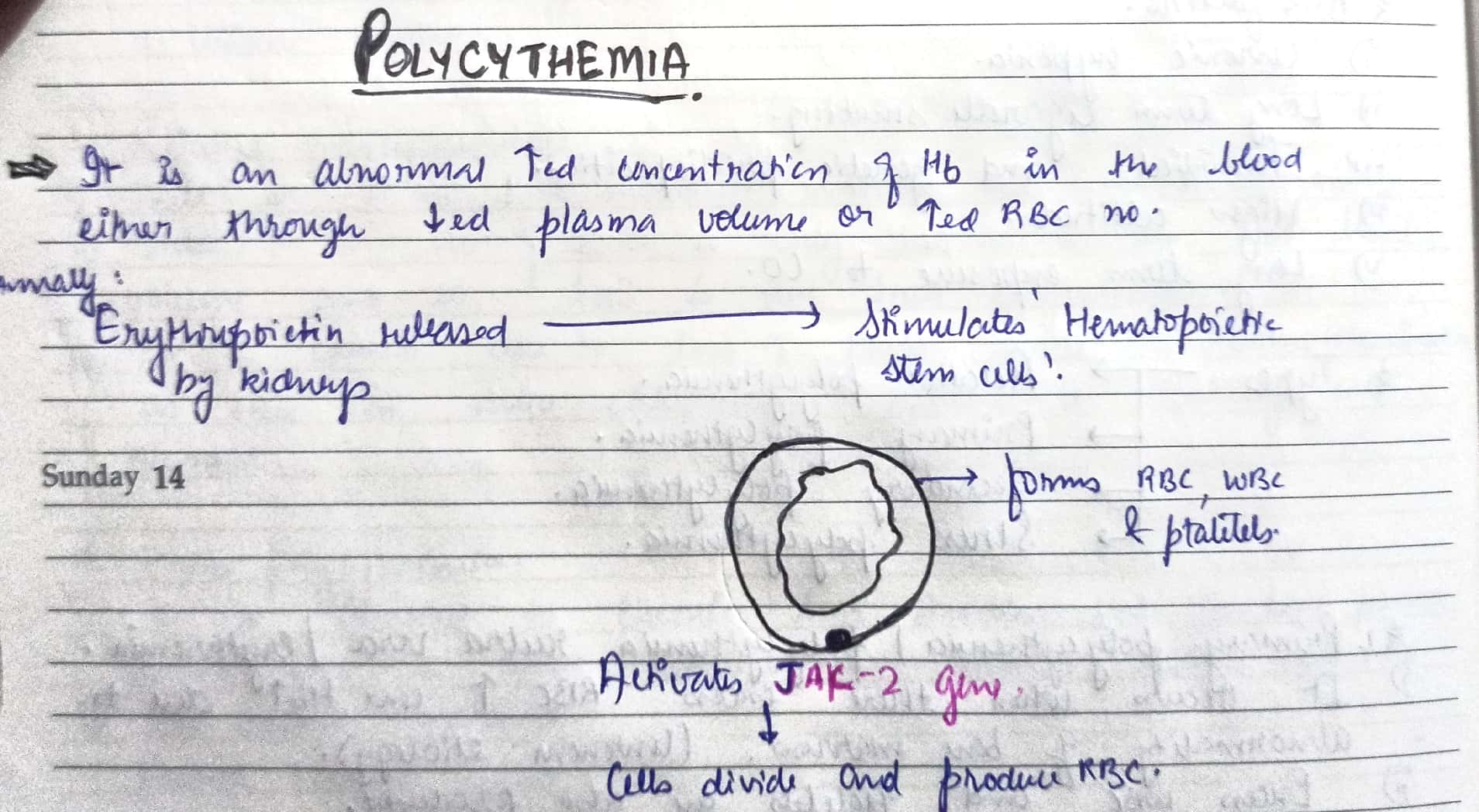
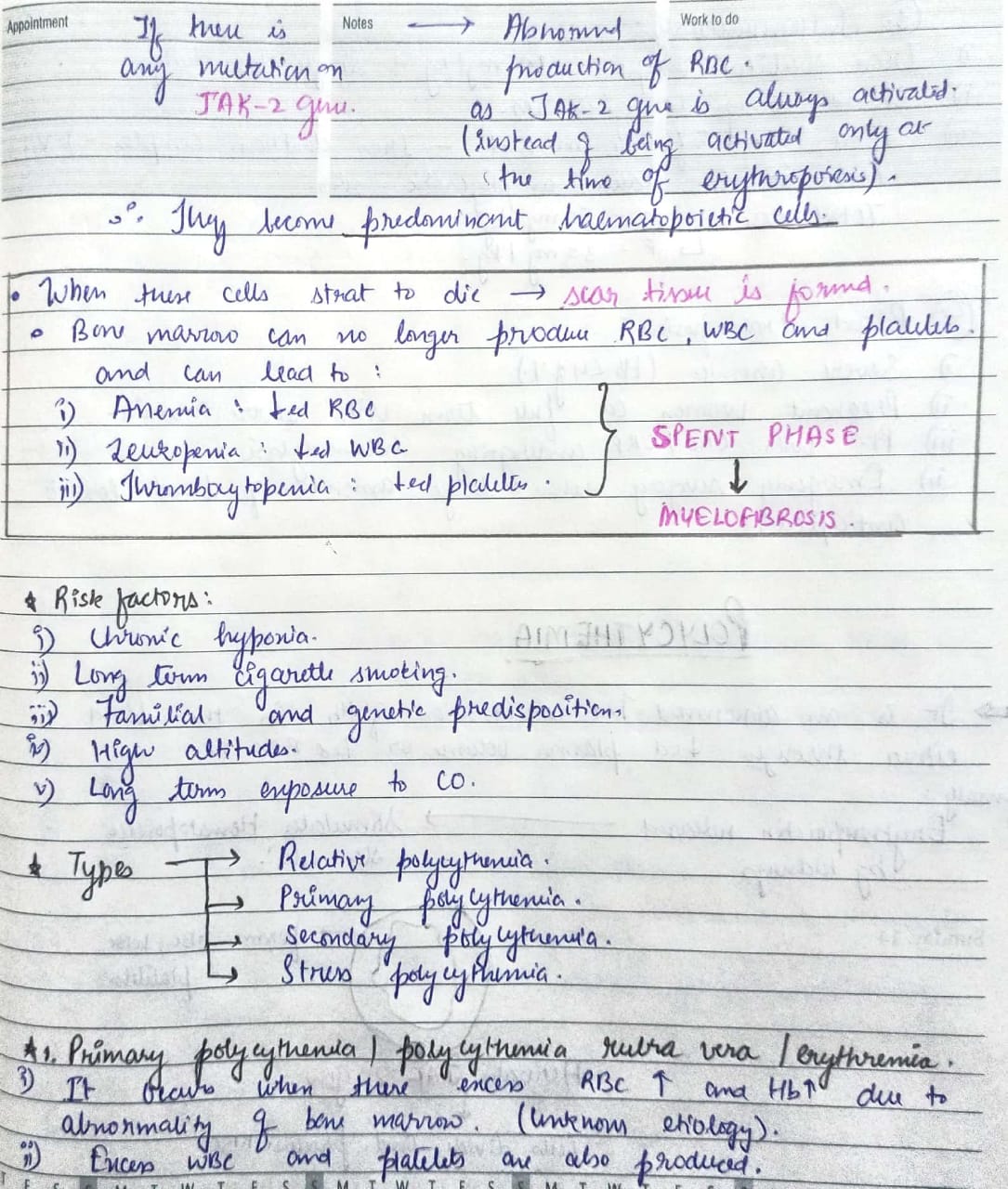
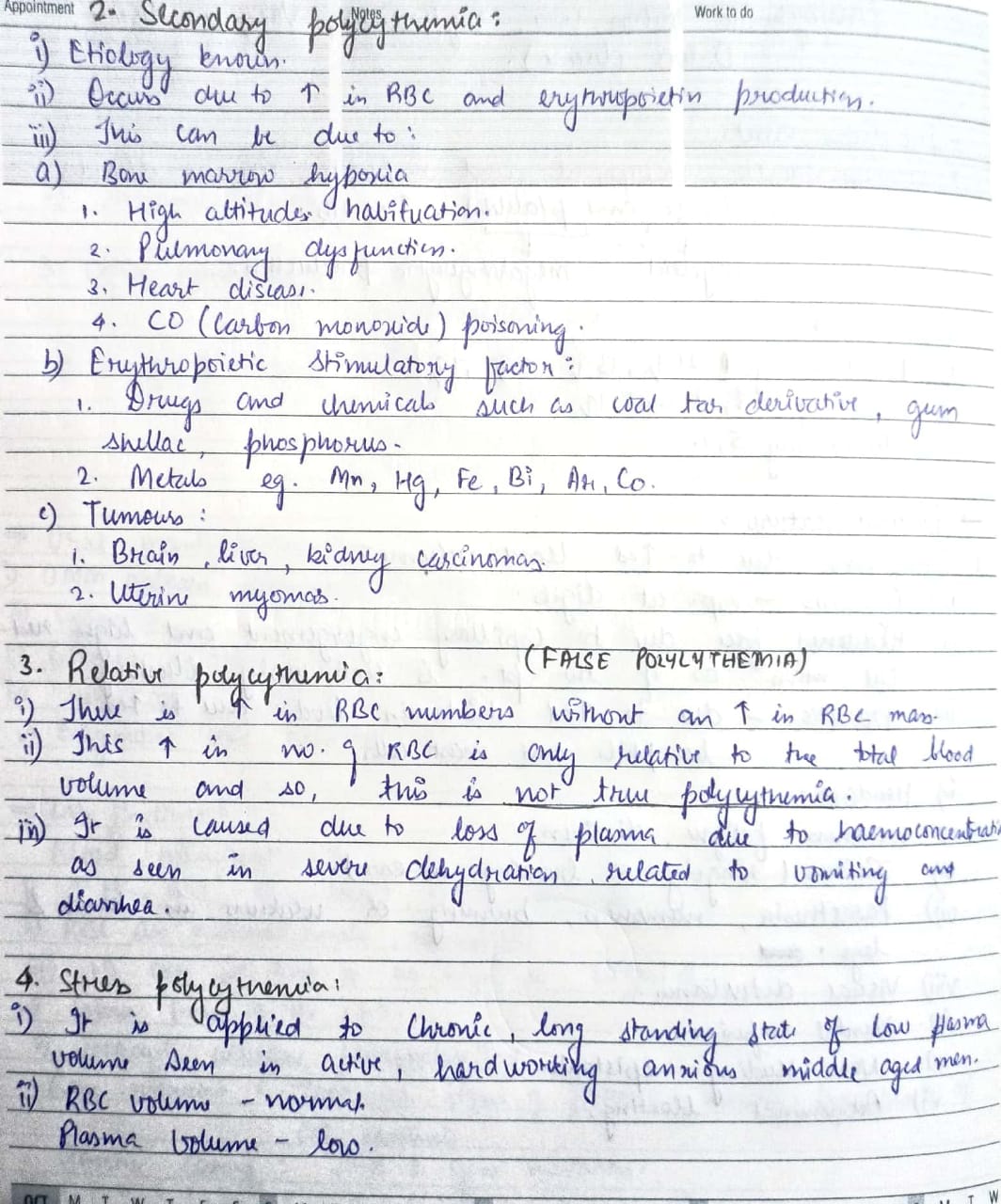
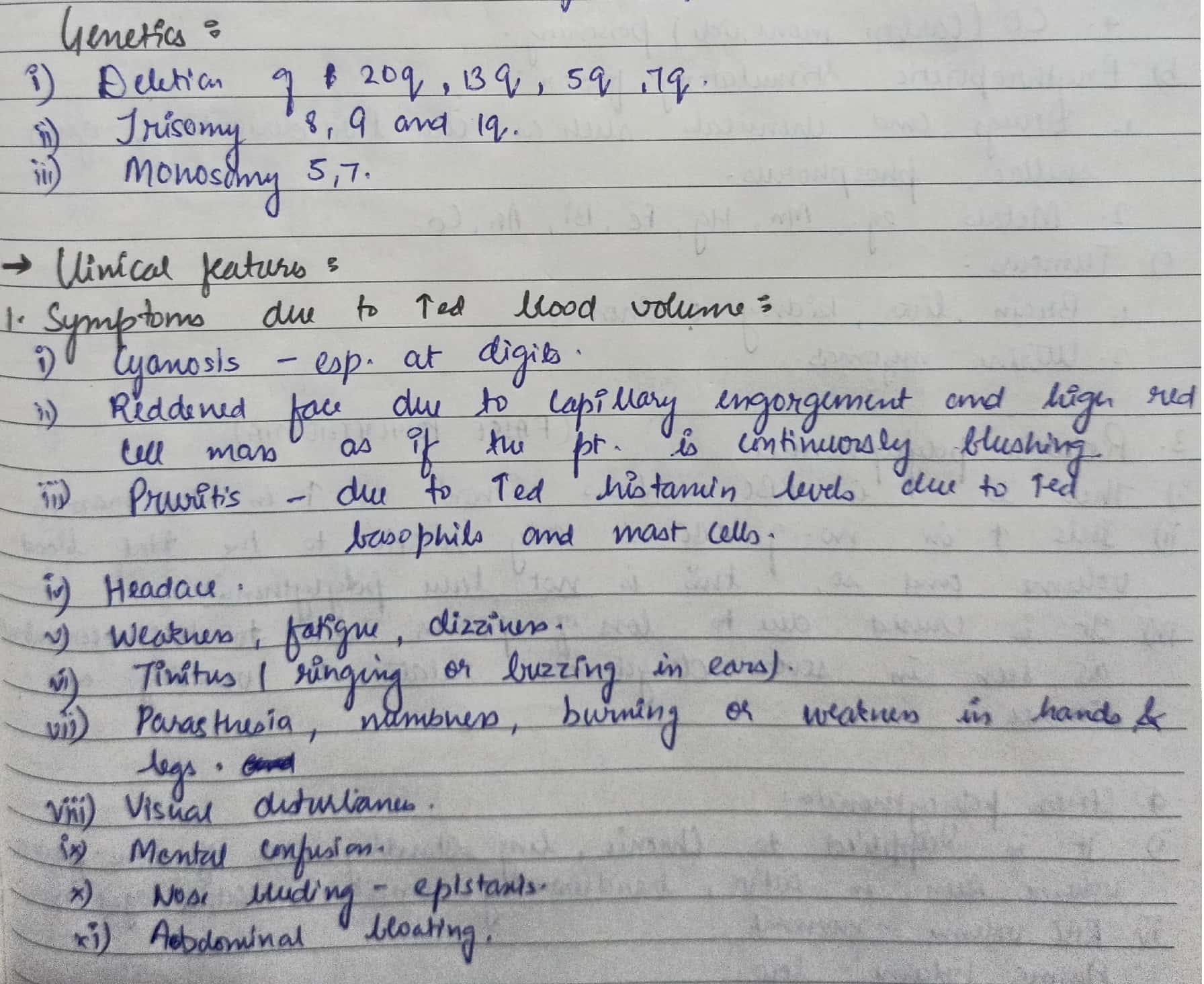
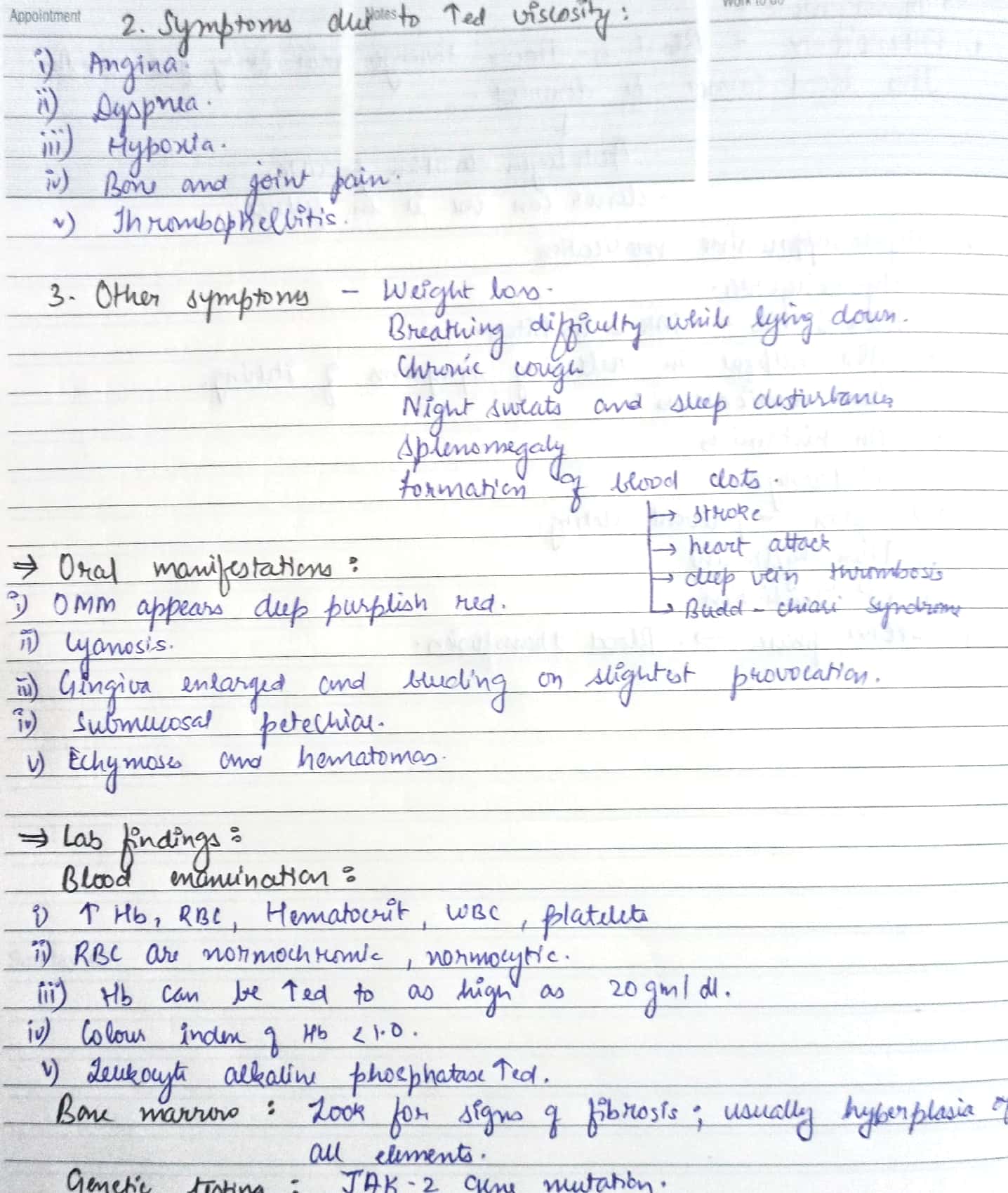
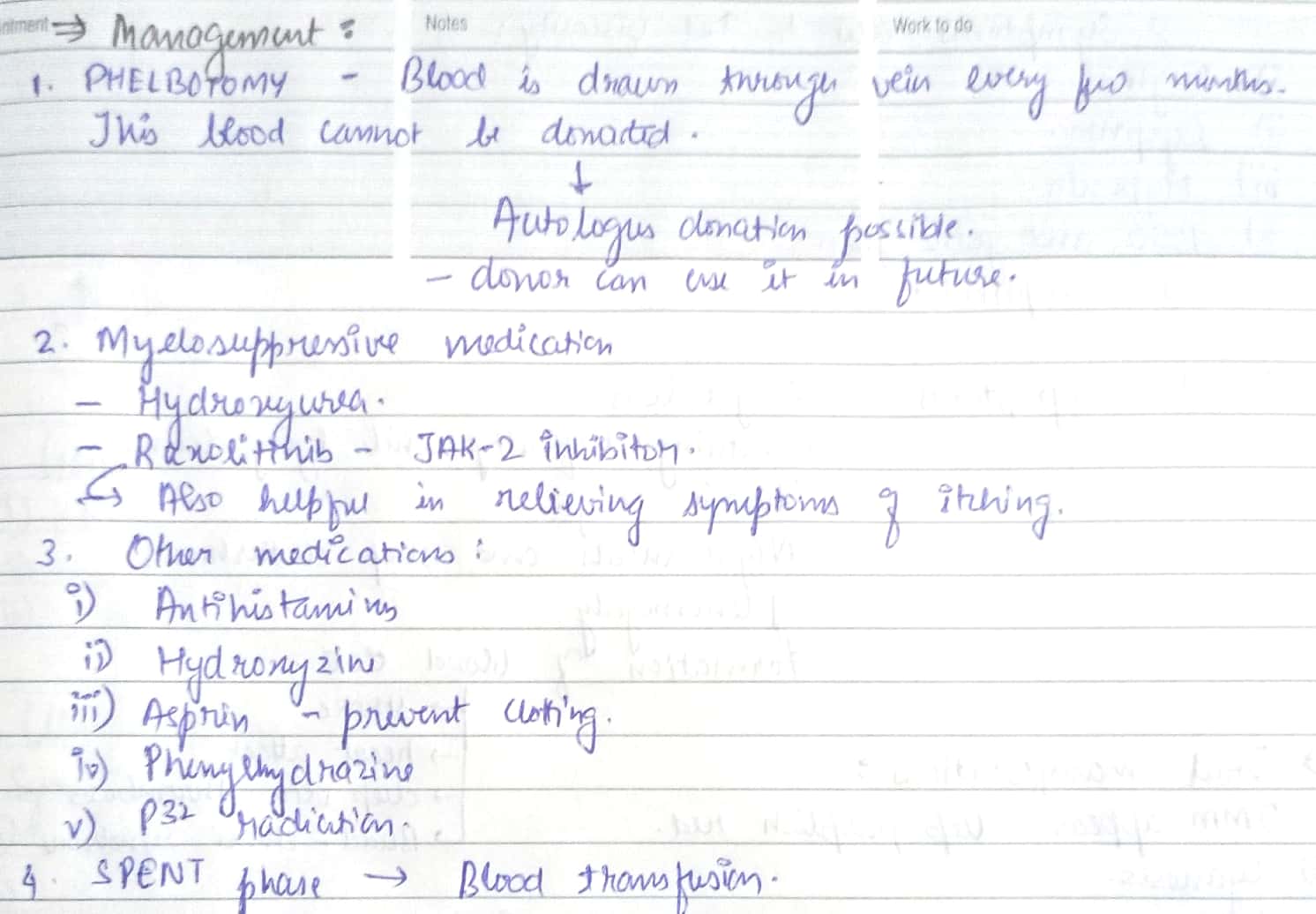
Polycythemia



References – Shafer’s textbook of oral pathology , SN Chugh Textbook of clinical medicine for dental students
Image reference : Google images
Plummer Vinson syndrome
Plummer Vinson triad :
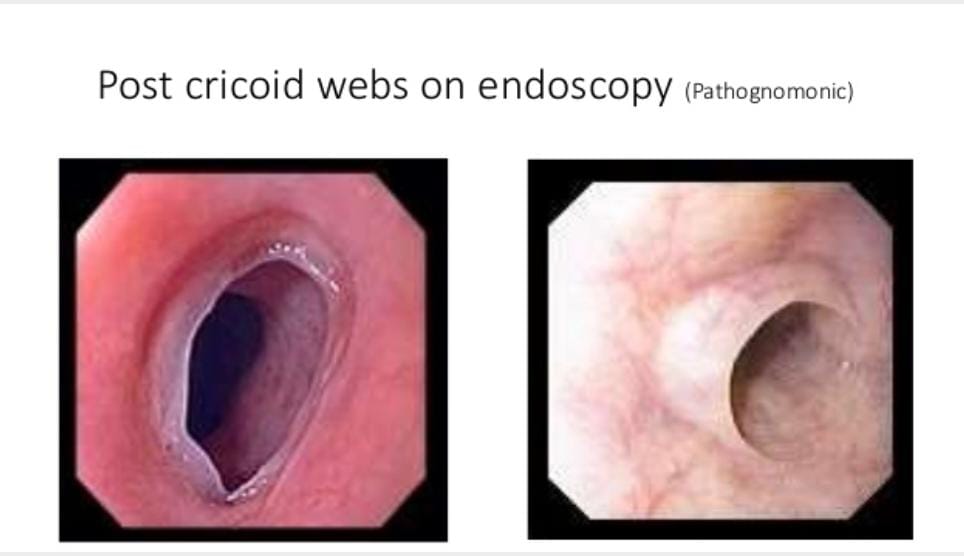
- Postcricoid dysphagia
- Upper esophageal webs
- Iron deficiency anemia
High risk of “squamous cell carcinoma”
Risk factors :
- Race – White and Scandinavian
- Age – 40-70 years
- Sex – Females more than males. Especially in postmenopausal women.
Pathophysiology :
- Iron deficiency anemia
- Nutritional deficiency
- Genetic predisposition
- Autoimmunity causes may include rheumatoid arthritis , pernicious anemia and thyroiditis.
Signs :
- Angular cheilitis
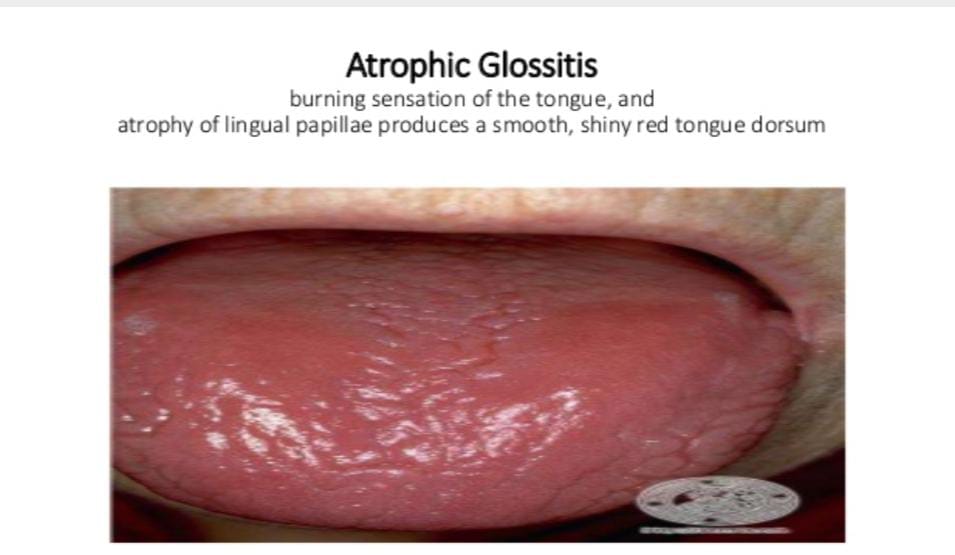
- Glossitis (Atrophic bald tongue)
- Pallor – Palmer pallor and conjunctival pallor
- Platynychia (Flattened nails)
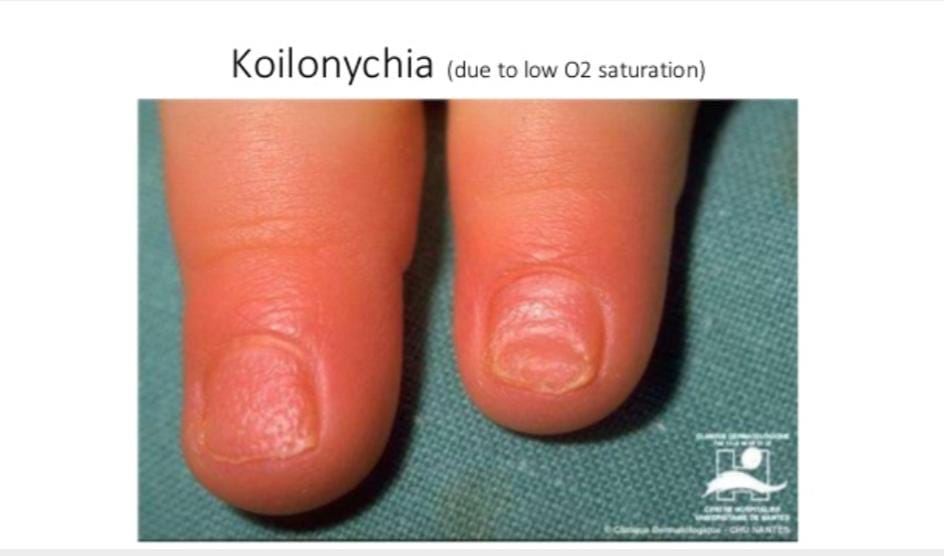
- Koilonychia (Spoon shaped nails)
- Splenomegaly
- Edentia (loss of teeth due to esophageal reflux)
- Enlarged nodular thyroid gland
- Gastritis with acholorhydia
- Post cricoid webs
- Picca
- Beeturia
- Restless leg syndrome
Symptoms :
- Dysphagia
- Odynophagia
- Choking spells and aspiration due to proximal location of webs
- Weakness and fatigue
- Weight loss
- Hair loss




References – Shafer’s textbook of oral pathology , SN Chugh – Textbook of clinical medicine for dental students , slideshare.com
Image reference : Google images.
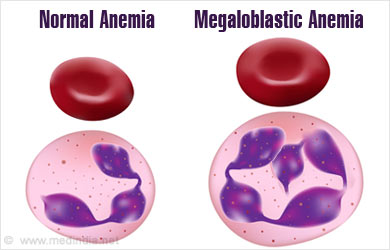
MEGALOBLASTIC ANEMIA
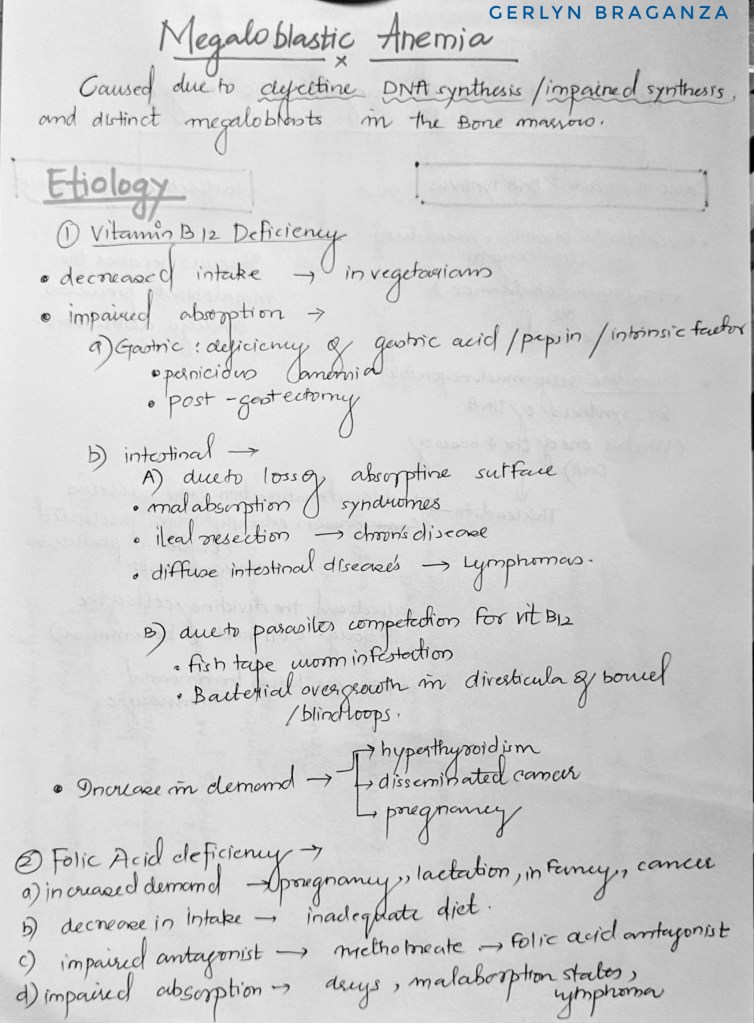
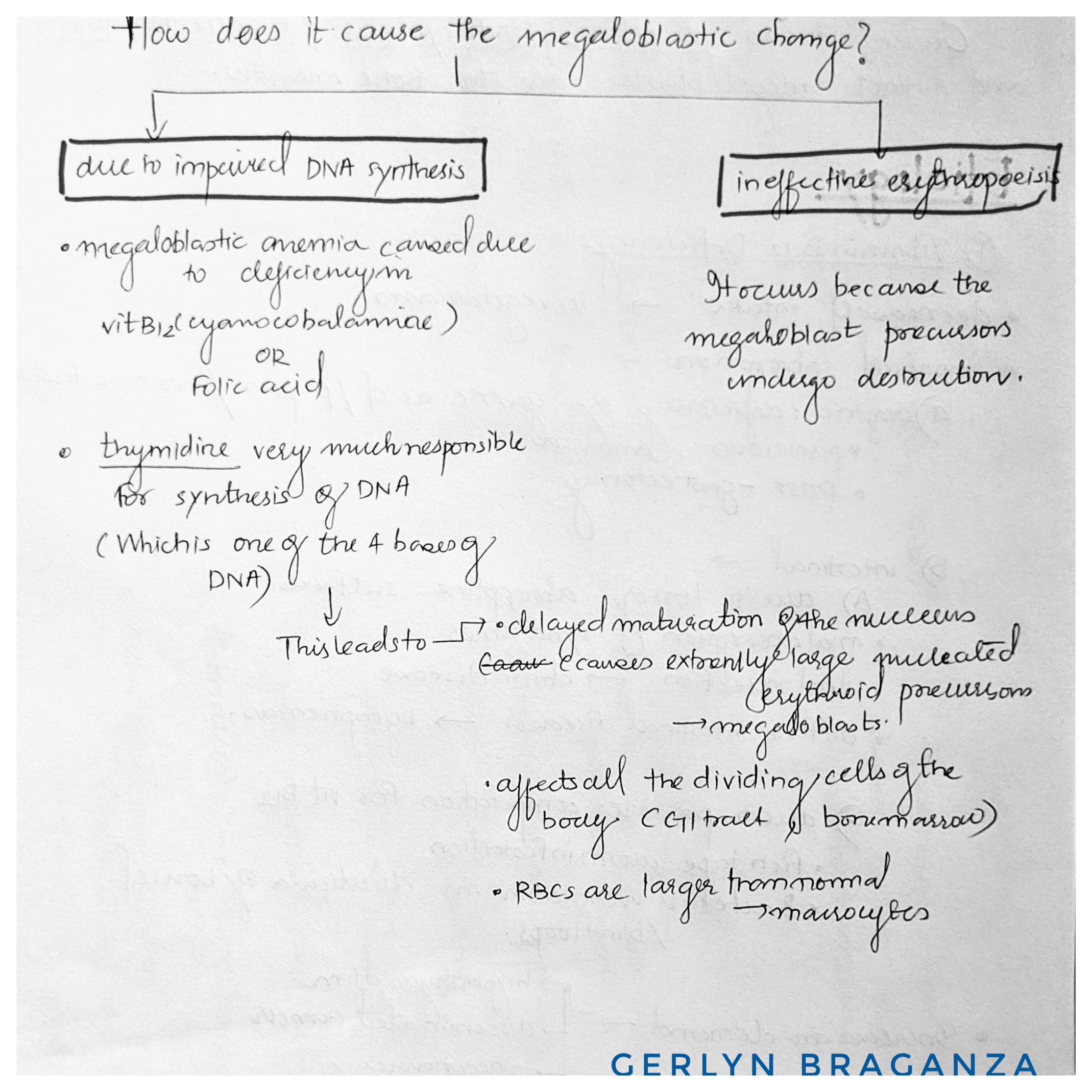

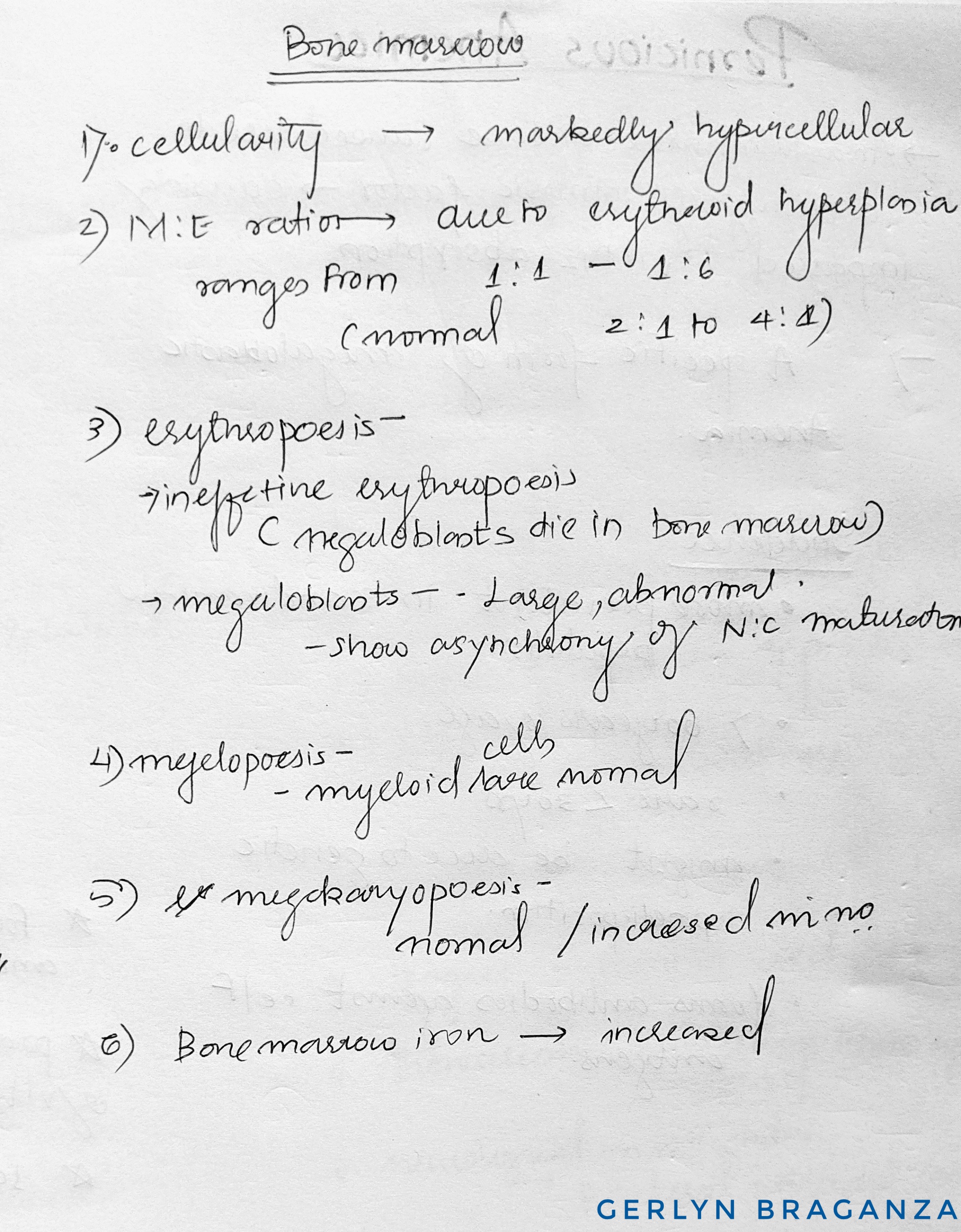
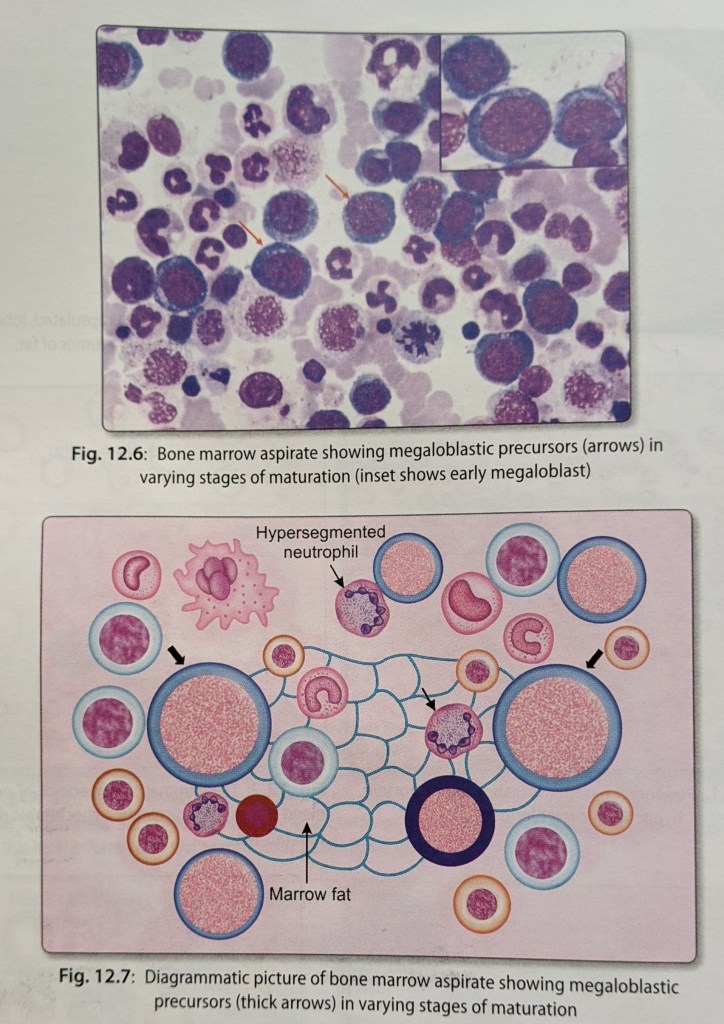
Source – textbook of pathology by ramdas nayak and harsh mohan
IRON DEFICIENCY ANEMIA
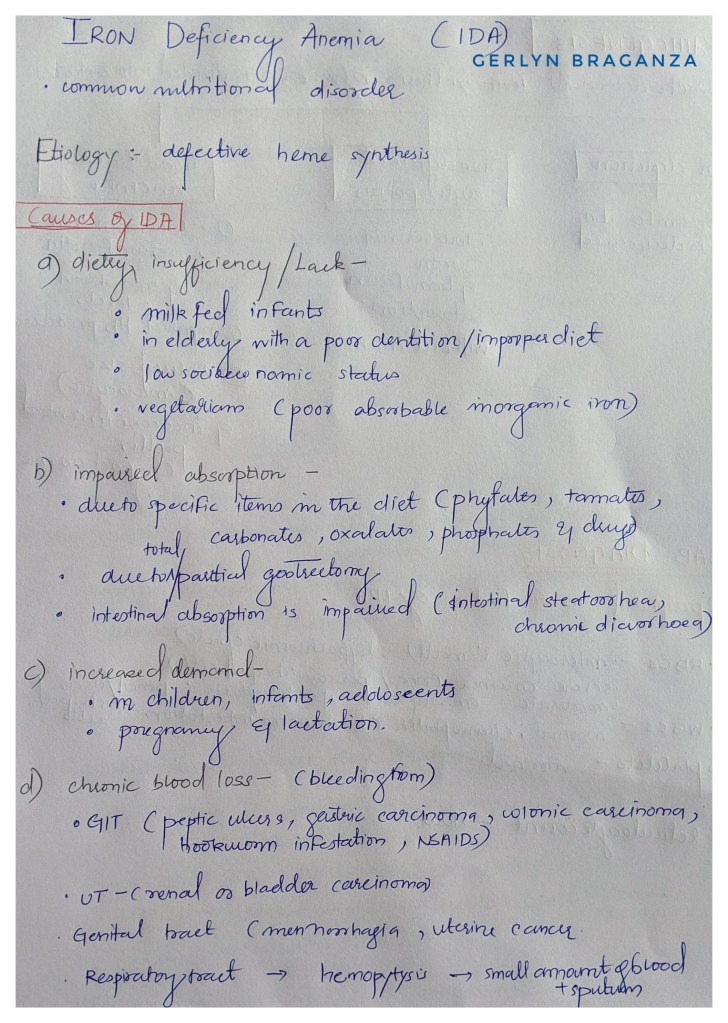


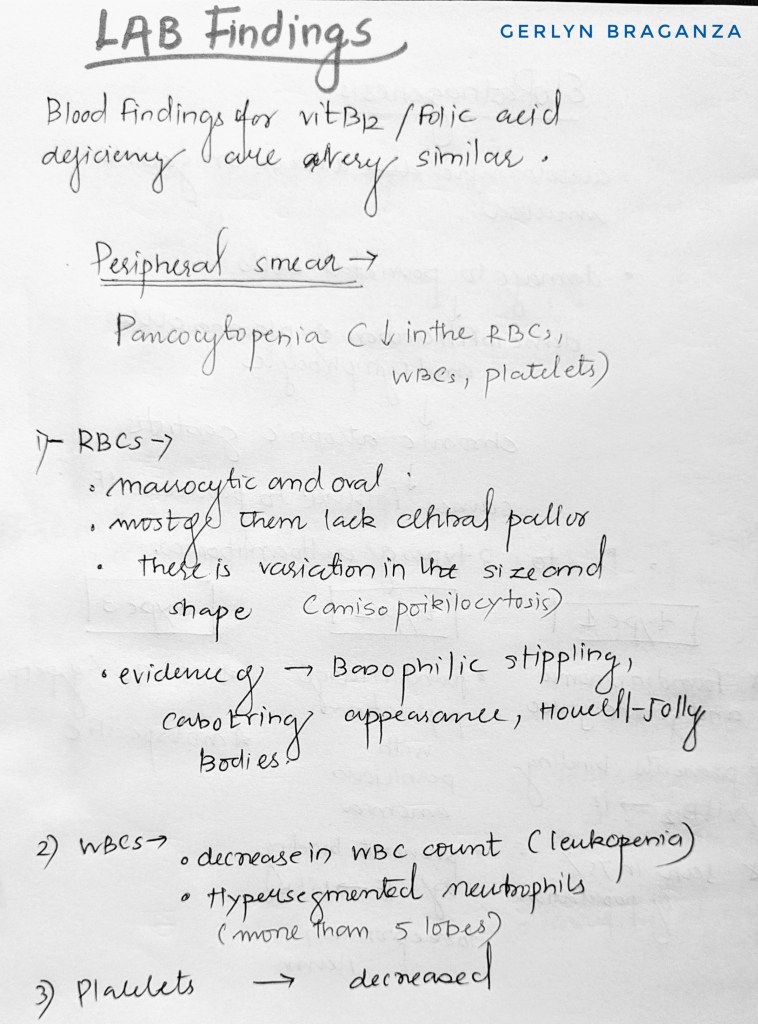
Peripheral smear
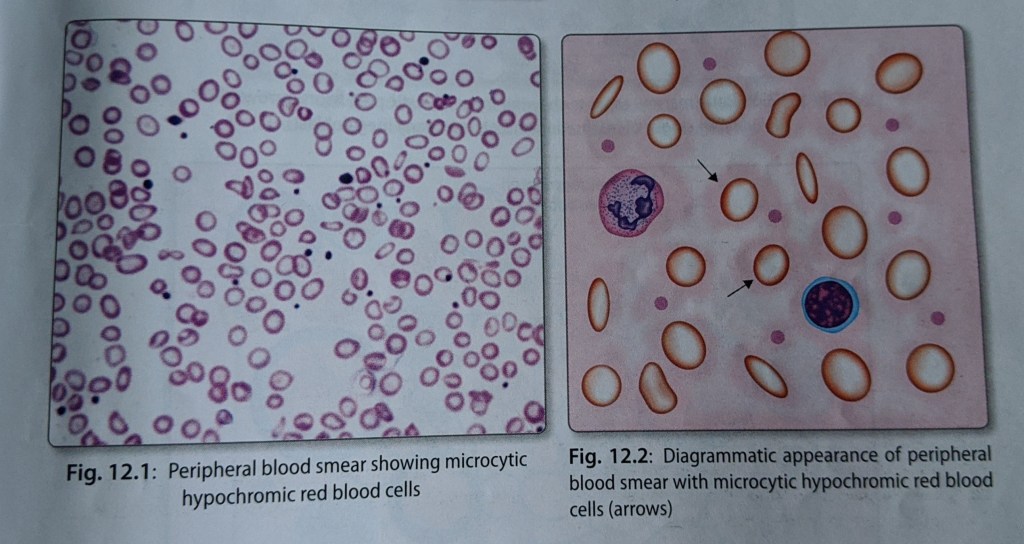
Reference – textbook of pathology for dental students – Ramdas Nayak
ANEMIA 🩸
Reduction of total circulating red cell mass below normal limits.
OR
Decrease in the oxygen carrying capacity of the blood that leads to tissue hypoxia.
Anemia may be absolute (decreased RBC mass), or relative ( associated with higher plasma volume).
Classification of anemia
1. Morphological classification
- Red red cell size ( normocytic, microcytic, or macrocytic)
- Degree degree of hemoglobinization( normochromic or hypochromic)
2. Etiological classification – given below in the tables
Morphological classification of anemia.

Etiological classification of anemia
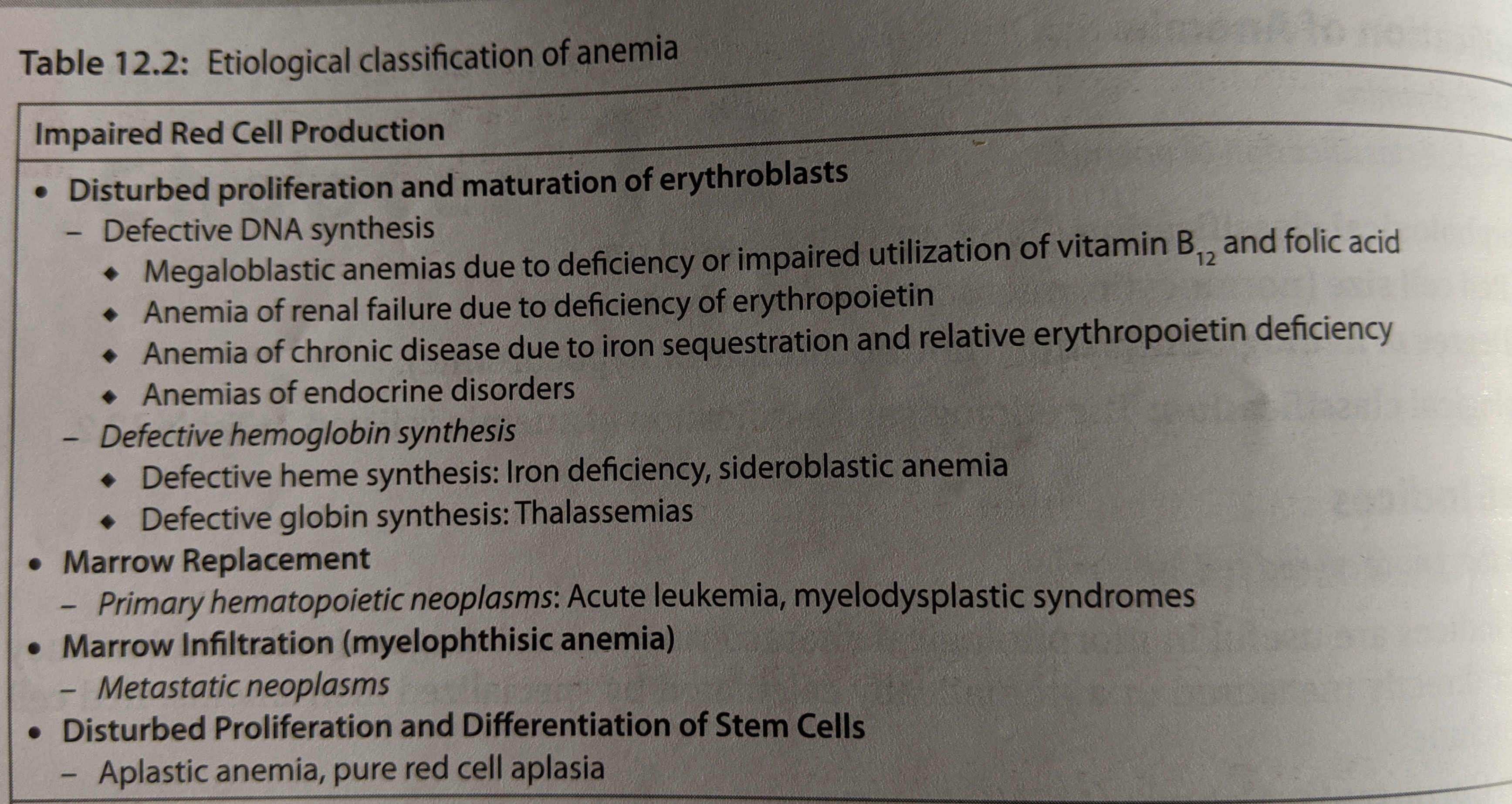

Source – textbook of pathology ( Ramdas Nayak )
Systemic Implications in Dental practice
Cyclosporine therapy may cause gingival hyperplasia
Gingival growth occurs in patients taking phenytoin.
Patients with cardiac disease should receive dental treatment in minimal stressful environment. Anxiety,exertion and pain should be minimized.
Irregular pulse, engorged jugular veins and tachypnea may indicate the presence of cardiac disease.A history of hypertension, ischemic heart disease or any other cardiac problem particularly congenital heart disease and drug intake (anticoagulant, aspirin) should be sought.Angina may present as pain in the mandible, teeth and other oral Tissues Epinephrine in the local anesthesia may raise the blood pressure and precipitate dysarrhythmias.In patients with IHD, facilities for medical help, oxygen and nitroglycerine should be Available General anesthesia should be avoided for at least three months in patients with recent onset angina
Patient’s with Cushing’s syndrome more prone to get infections.(candidiasis)
Elective dental surgery should be deferred for 6 months following acute MI.Prophylaxis for infective endocarditis is mandatory in cases where there is a risk.Cardiac patients on anticoagulant drugs or aspirin are at increased risk of bleeding following dental procedures.Hence, these drugs should preferably be stopped a week before the procedure.Calcium channel blockers may cause gingival swelling and lichenoid lesions in the oral cavity. ACE inhibitorscan cause loss of taste, burning sensation in oral cavity,and angioedema. Dry mouth can result due toantihypertensive drugs such as d
Rifampicin can cause red saliva.
Elective dental care is avoided in patients with acuterenal failure
Elective dental procedures are better tolerated on non-dialysis days
Blood pressure measurement is advised at every visit.
Brown to black macular pigmentation in oral mucosa can be suspected for Addison disease.
Gonorrhea may present uncommonly with oral manifestations like tonsillitis, lymphadenitis, and painful oral and pharyngeal ulcers.
Oral manifestations in peptic ulcer disease are rare.However erosive dental lesions could be appreciated on lingual surface of lower incisors or palatal surface of upper maxillary teeth.
Neoplasm Histopathology
OVERVIEW
- The basic components of a tumor are the parenchyma and stroma.
— The parenchyma comprises the neoplastic cells.
— The stroma comprises the supporting connective tissues, blood vessels, and immune cells. - Interactions between these components determine the growth and behaviors of the neoplasm.
- Benign tumors are localized, organized, and tend to display slower growth.
— Because of these characteristics, benign tumors are typically amenable to surgical removal, which may be necessary when benign tumors grow large enough to impair functioning of the surrounding tissues. - Malignant tumors are invasive, disorganized, and often grow erratically; they are potentially metastatic, which means they can cross anatomical boundaries.
BENIGN
- Benign tumors are often named by combing the cell type of origin with the suffix “-oma;” however, some important exception to this rule are the malignant tumors of lymphoma, mesothelioma, and melanoma.
Adenoma of the thyroid gland
- Well differentiated, which means that the tumor cells resemble that of the normal thyroid gland.
- It is functional, as we can see numerous colloid-filled follicles.
- Relatively normal looking nuclei.
Pancreatic tissue with serous cystadenomas
- Microcysts
- The pancreatic acini are relatively normal looking.
- Serous cystadenomas are also often commonly found in the ovaries.
Squamous papillomas on the tongue
- Numerous macroscopic fingerlike and warty projections.
- When such projections extend into a lumen, they are called “polyps.”
MALIGNANT
- Sarcomas are malignant tumors that form in sold mesenchymal tissue, such as bone, fat, and muscle.
- Leukemias and lymphomas are cancers of the white blood cell lines.
- Carcinomas are tumors that form from epithelial cells, such as in the skin or the internal linings of the organs.
— Squamous cell carcinomas: the tumor cells look like stratified squamous epithelium, and,
— Adenocarcinomas: the tumor cells grow in a glandular pattern. - “Undifferentiated malignant tumors” are those of unknown tissue origins.
Adenocarcinoma in the colon
- It is anaplastic, that its, it is not well differentiated. The glandular tissue that has proliferated is not like that of the normal colon mucosa.
- See image of a large polyp growing from the wall of the colon; even if this wasn’t a malignant tumor, we can see how this would obstruct normal bowel functioning.
Oral squamous cell carcinoma
- Pleiomorphic cells, which range from small to giant.
- Large, hyperchromatic nuclei.
- Several of the cells are in various stages of mitosis, reflective of their hyper-proliferative state.
Thyroid adenocarcinoma
- The malignant tumor is anaplastic and disorganized.
- It is nonfunctional, which we can see from the absence of colloid-filled follicles.
Metastatic brain tumor
- It has irregular edges without a distinct enclosing capsule, which lends to its invasive nature.
Some special cases
- Mixed tumors
The parenchymal cells of most tumors are uniform; however, denote that mixed tumors comprise multiple cell types.
For example, a mixed tumor of the salivary gland may comprise epithelial cells as well as other types not typically found in the gland. - Teratomas
The cells of most neoplasms are derived from a single germ cell layer; however, denote that teratomas comprise cells and tissues from multiple germ layers.
For example, we can see multiple tissue types in an ovarian teratoma, even hair and tooth-like structures.
Cancer – Mutations & Model of Development
CANCER
- Cells reproduce in defiance of restraints
- Cells invade and colonize territories reserved for other cells
Benign tumors
Reproduce without restraint but are noninvasive
Malignant tumors
Reproduce and metastasize
Proto-oncogene
Gene whose protein product stimulates normal cell growth and division
Oncogene
Mutated gene that has hyperactive function that can lead to cancer
Tumor suppressor gene
Gene whose protein product inhibits cell division and whose mutation can lead to cancer if it leads to decreased function
4 TYPES OF CANCER CAUSING MUTATIONS
Proto-oncogene
- Gene moves to new location
- Could lead to excess protein production
- Gene is duplicated
- Could lead to excess protein production
- Mutation in gene’s control element
- Could lead to excess protein production
- Mutation in gene itself
- Could lead to hyperactive or degradation resistant protein
MULTISTEP MODEL OF CANCER DEVELOPMENT
- Cancer is caused by an accumulation of mutations, not just one
Example: colon cancer pathway
- Loss of tumor suppressor function (adenomatous polyposis coli gene)
- Can lead to a polyp (benign growth)
- Activation of ras oncogene and
- Loss of another tumor suppressor gene
- Can lead to an adenoma (larger benign growth)
- Loss of p53 tumor suppressor and
- Addition mutations that allow for invasion and metastasis
- Can lead to carcinoma (malignant tumor)
Apoptosis
- Programmed cell death
- Specific biochemical signature (ex. phosphatidylserine “flips” to outer surface of plasma membrane)
- Does not induce inflammation
Important in a Variety of Processes
- Organism development
- Cell number and organ size
- Quality control during development
- Removal of damaged cells
Cellular Changes
- Cytoplasm condenses
- Nucleus becomes misshapen
- Chromatin condenses along the nuclear envelope
- Cell eventually fragments into blebs
- Phosphatidylserine on the blebs indicates to phagocytic cells that apoptosis is occurring
- Phagocytic cells clear the cellular debris
Two Paths of Apoptosis
- Extrinsic Pathway (using the Fas pathway as an example)
a) Trimeric Fas ligand on another cell binds to Fas death receptor
b) Intracellular domain of Fas receptor recruits and activates FADD (Fas associated death domain)
c) Activated FADD recruits initiator procaspases such as procaspase-8 or -10 (complex is referred to as death-inducing signaling complex or DISC)
d) Complex formation activates the procaspases which then activate executioner caspases
e) Executioner caspase activation leads to apoptosis
- Intrinsic Pathway
a) Apoptotic stimulus activates BH3-only protein
b) BH3-only protein blocks the activity of Bcl-2 protein
c) Without Bcl-2 activity, BH123 proteins are able to oligomerize and cytochrome c is released from the intermembrane space of mitochondria
d) Cytochrome c in the cytoplasm activates Apaf1 proteins which form a heptameric complex
e) Apaf1 complex recruits initiator procaspase-9
f) Activated caspase-9 activates executioner caspase
g) Executioner caspase activation leads to apoptosis
Bcl-2 Family of Proteins
- Based on which specific domains are present in the protein
- Anti-apoptotic Bcl-2 proteins (ex. Bcl-2 or Bcl-XL)
- Pro-apoptotic BH123 proteins (ex. Bax or Bak)
- Pro-apoptotic BH-3 proteins
