source – don’t remember, had written it a lot time ago
Category: General Medicine
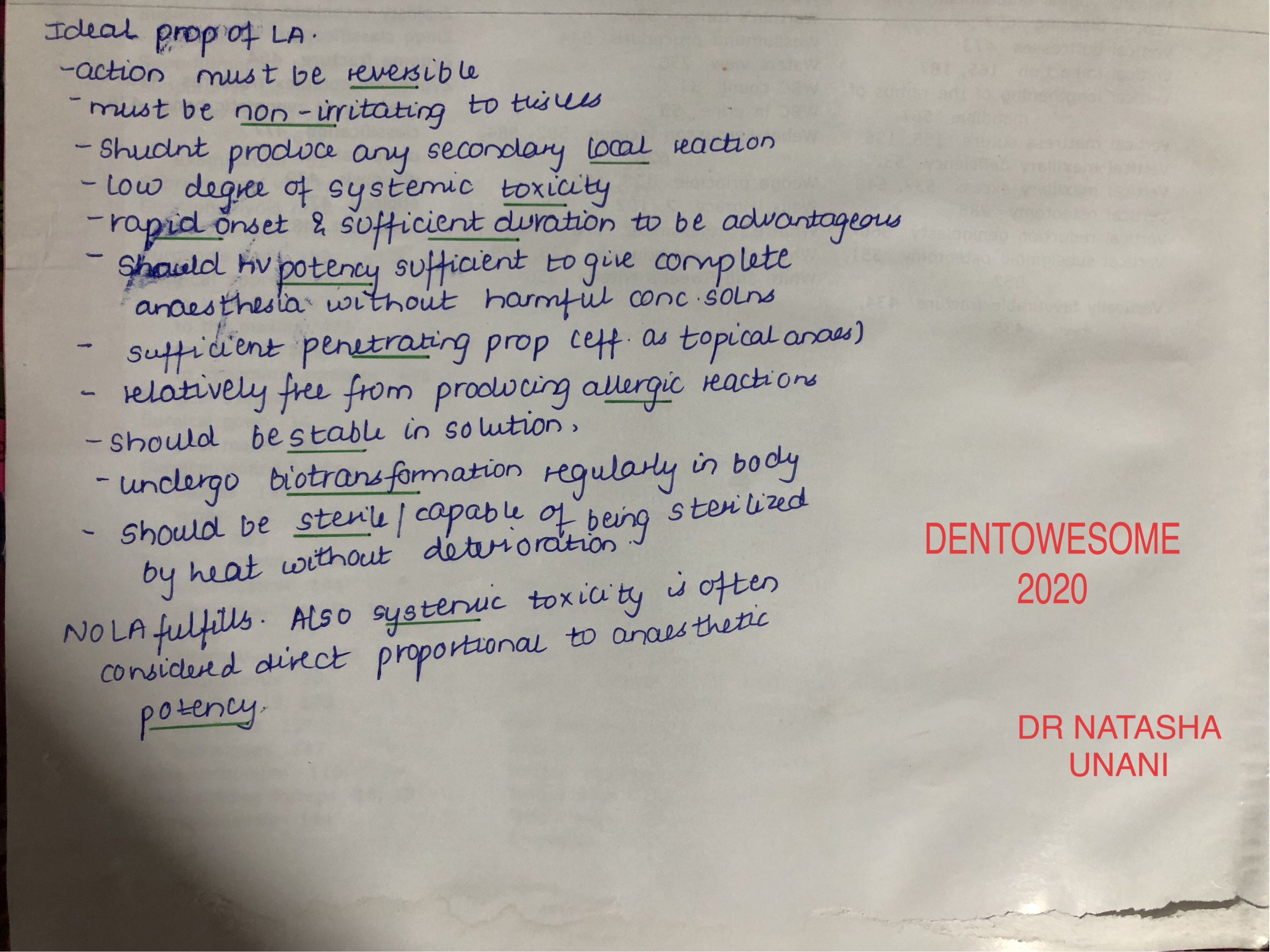
IDEAL PROPERTIES OF LA
source – don’t remember, had written it a lot time ago
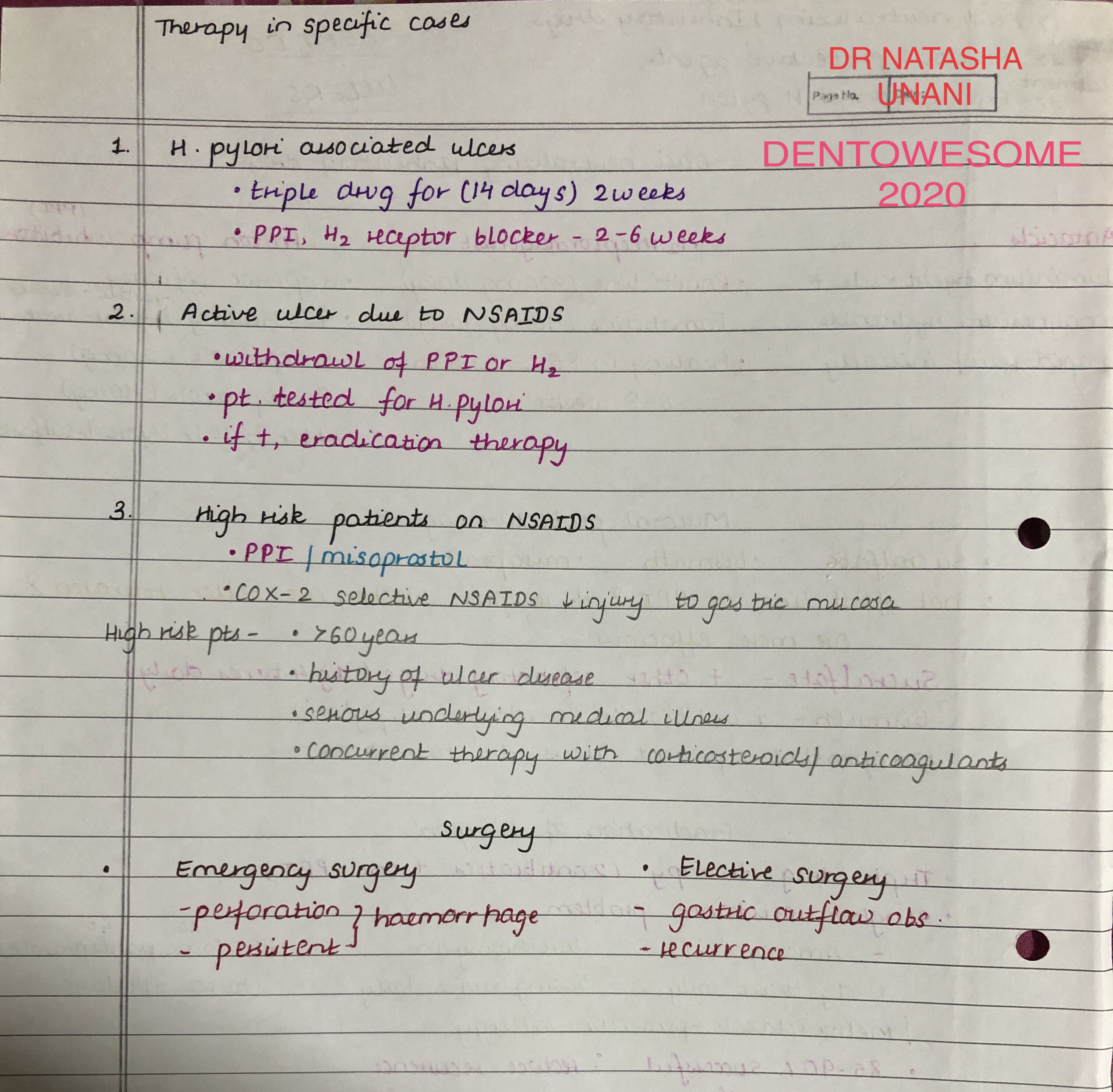
PEPTIC ULCERS

source – don’t remember, had written it a lot time ago
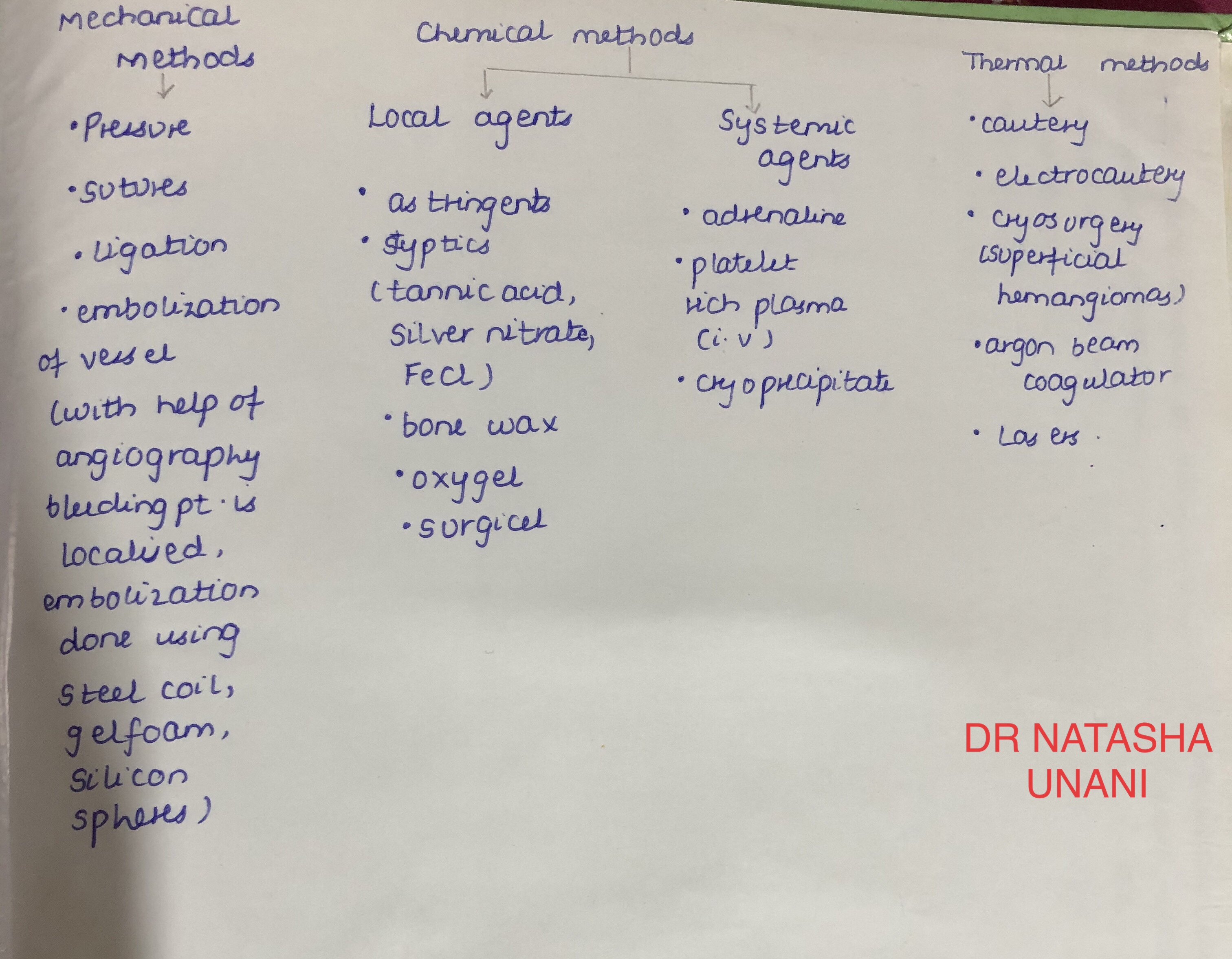
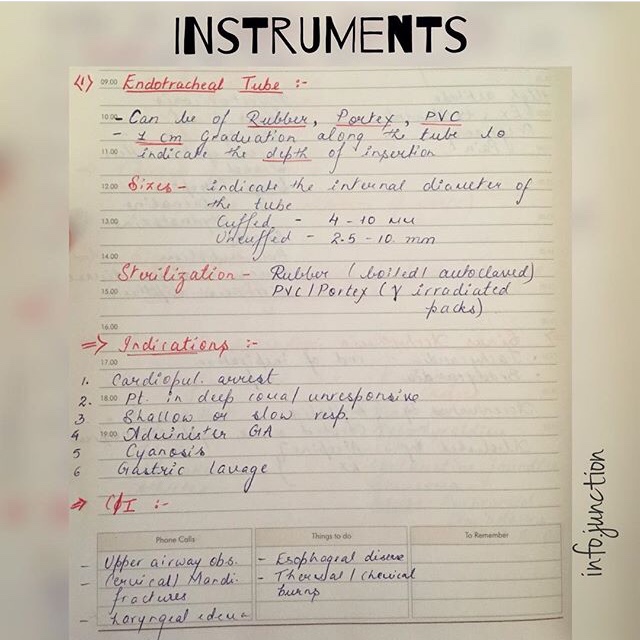
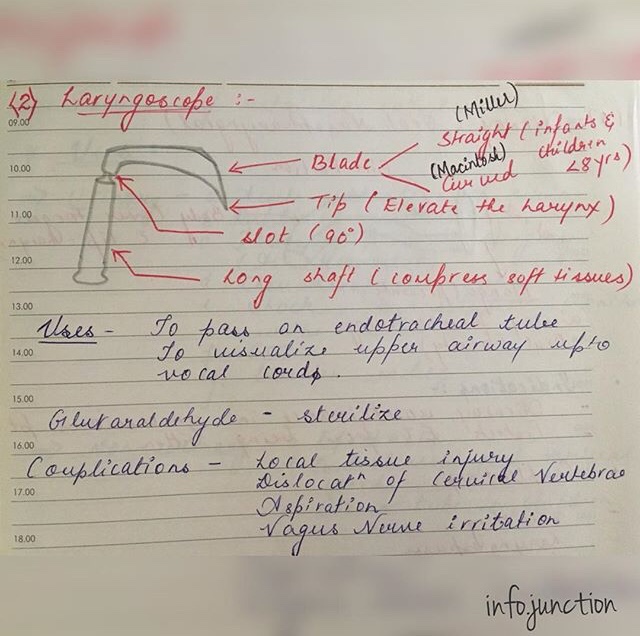
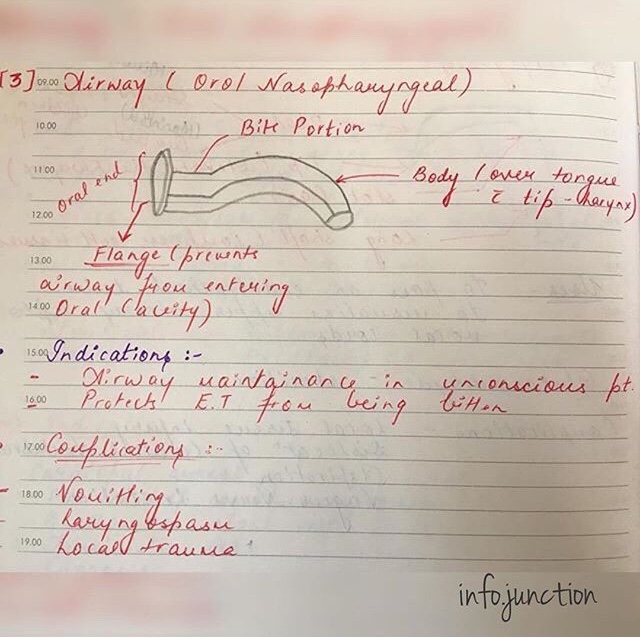
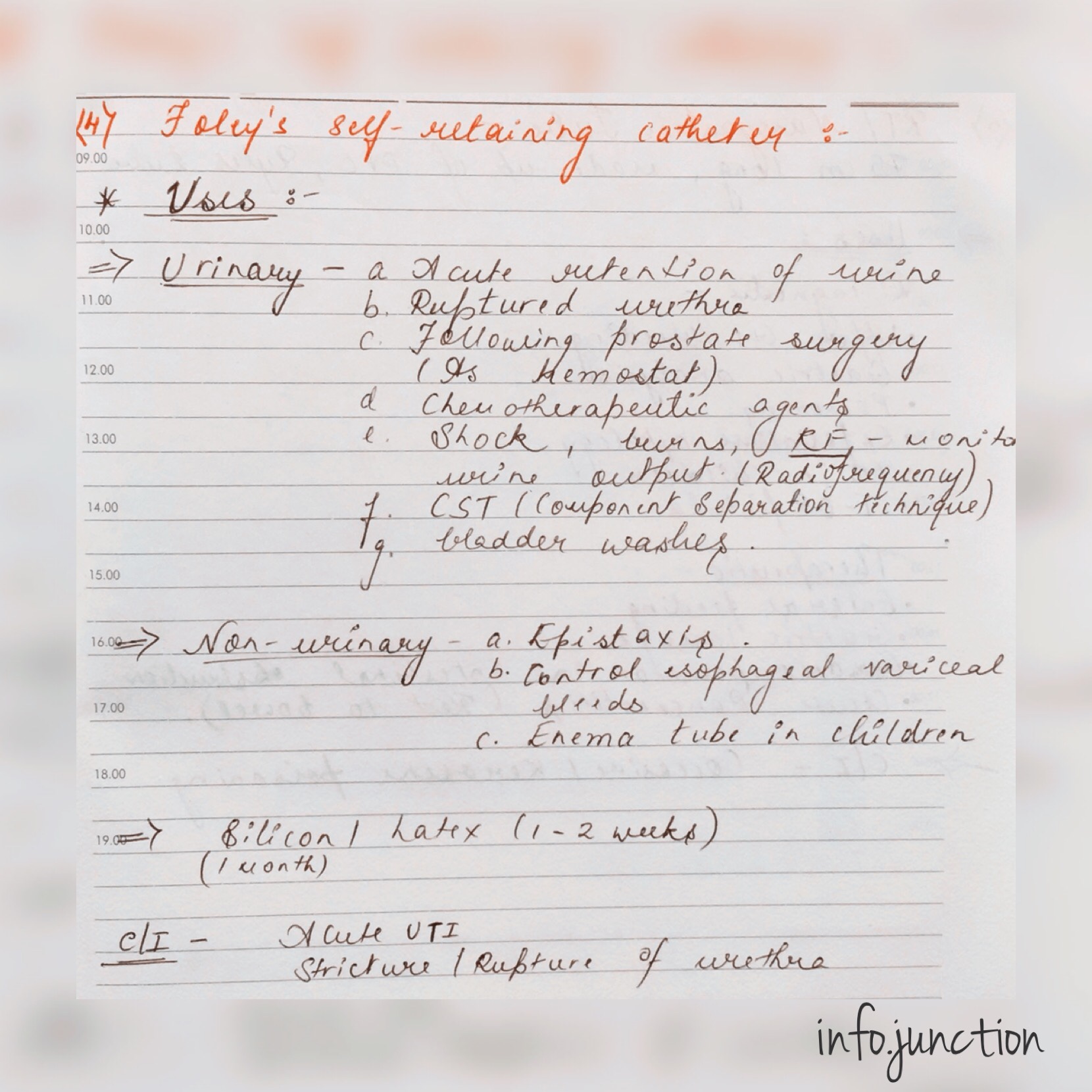
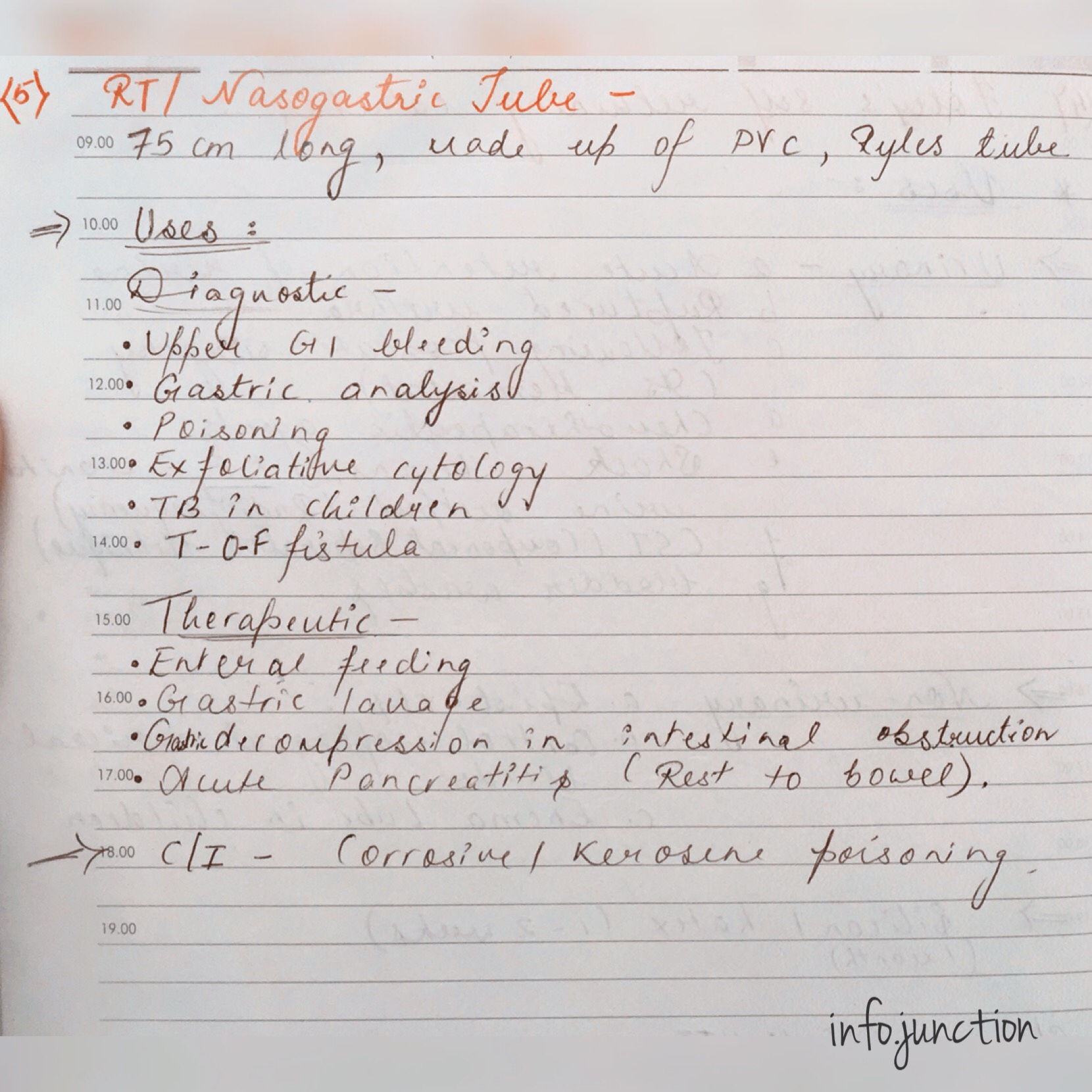
EMERGENCY INSTRUMENTS-II
1) 3-way: It consists of two inlets & one outlet.
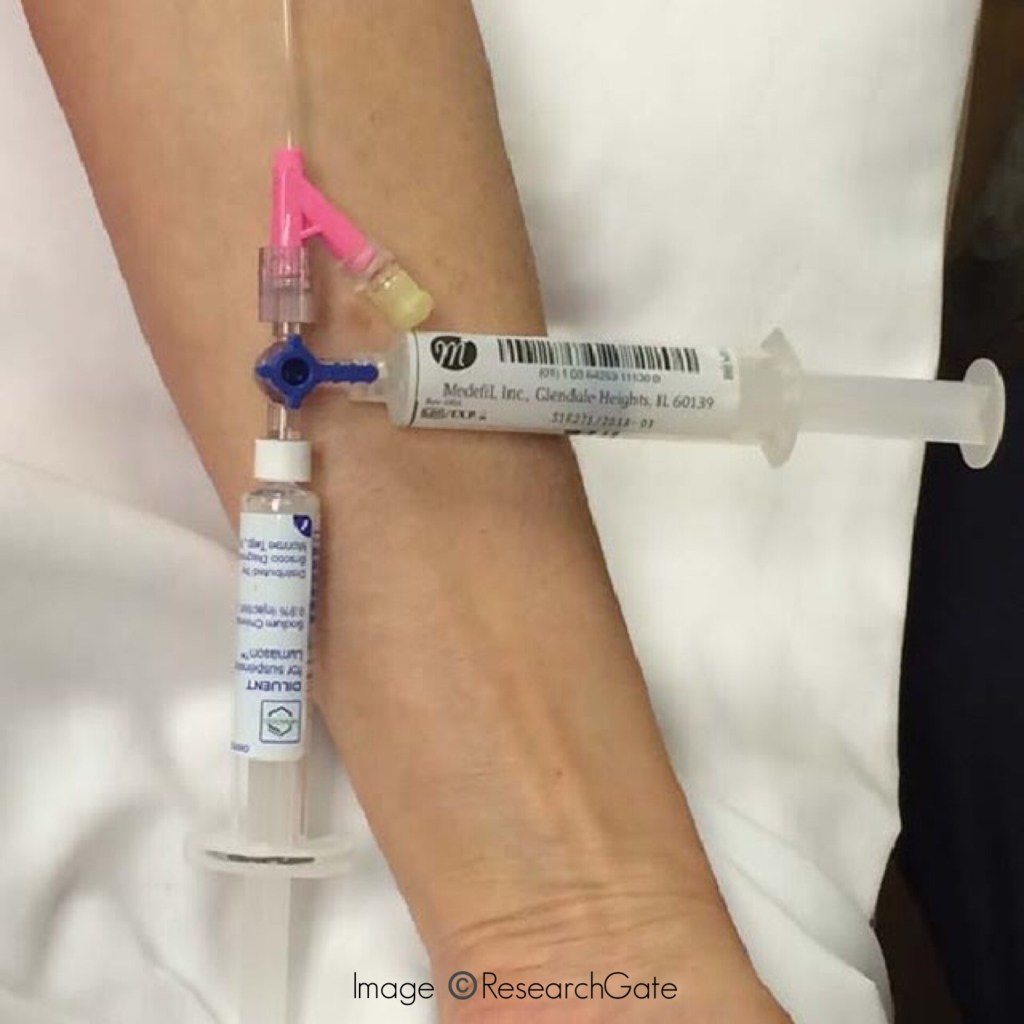
Uses:
- It is commonly connected to the IV cannula where through one inlet IV fluids pass and through the other inlet medications can be given or Central venous pressure(CVP) can be monitored.
- Aspirating fluid from the body cavities.
- Exchange transfusion.
2) IV cannulas:
Size: 14G – 24G (Smaller the no., larger the bore of the needle)
Use:
- Venous access for longer period.
- IV fluids
- Drugs administration
- Collection of blood samples
Source: Internet
EMERGENCY INSTRUMENTS-I
@dr.mehnaz
References: Practical Medicine by P.J Mehta
RESPIRATORY FAILURE

source – don’t remember, had written it a lot time ago
RESPIRATORY SYSTEM
🔹EXAMINATION:
A. Inspection & Palpation:
Normal ⬇️
- Bilaterally Symmetrical
- Ellipsoidal in shape
- Transverse diameter > Antero-posterior diameter
- Acute subcostal angle
▪️Abnormal shapes of chest:
1) Pigeon Breast/Keeled chest – Rickets

- Ricketic Rosary – cartilagenous overgrowth at costochondral junction.
- Harrison sulcus – indrawing of soft ribs during inspiration.
2) Funnel Chest/Cobbler’s chest –
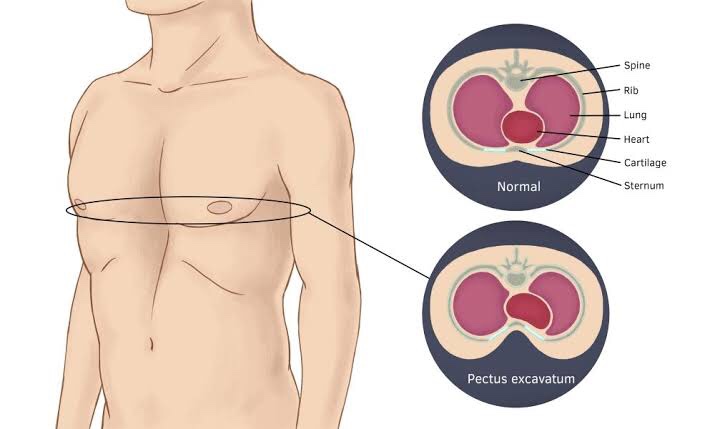
Image©️healthand.com

3) Barrel shaped chest – Emphysema
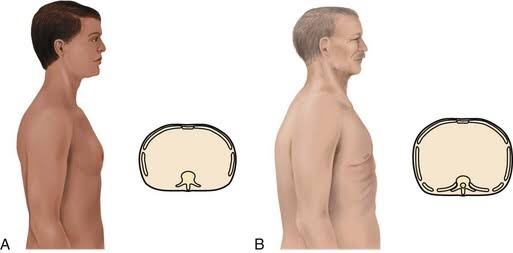
- Increased A-P diameter, wide subcostal angle
- Sternum more arched
- Spine – concave
- Ribs – less oblique
4) Spinal Deformities – Scoliosis

Alar Chest – In advanced TB, scapula is winged
▪️Respiratory Rate:
Range: 16 – 20 beats/min.

▪️Respiratory Rhythm:
1) Cheyne-Stokes Respiration:
➡️ Alteration of apnea & hyperpnea due to anoxemia. Therefore CO2 accumulation in body causing hyperventilation.
➡️ Causes:
- Left ventricular failure(LVF)
- ⬆️ Intracranial pressure(ICP)
- Poisoning
- Uremia
- Deep sleep
2) Kausmaul’s Breathing:
- Air hunger(Rapid & Deep)
- Diabetic Ketoacidosis, alcoholic, starvation, uremia
3) Bitot’s Respiration: Meningitis
▪️Type of breathing:
- Abdominothoracic – males
- Thoracoabdominal – females
- Thoracic – Severe Ascitis
- Abdominal – Collapse of lung
▪️Movements:
Unilateral diminished movement–
- Pleural effusion
- Consolidation
- Fibrosis
Bilateral movement–
- Bronchial Asthma
- Emphysema
▪️Mediastinum:
➡️ Shift detected by noting position of Trachea (suprasternal notch) / Apex beat (5th Inter-costal space)
➡️ Trail’s sign: It is the undue prominence of the clavicular head of sternomastoid on the side to which the trachea is deviated.
▪️Vocal Fremitus:
➡️ Tactile perception of viberations to chest wall from larynx during act of phonation.
- Increased – consolidation
- Decreased – Pleural effusion, pneumothorax, Asthma, fibrosis, collapse, emphysema
B. Percussion:
➡️ Normal: Resonant
- Impaired – ⬇️ air in lungs
- Dull, stony dull note (effusion)
- Tympany (emphysema, pneumothorax)
➡️ Normal liver dullness –
The “5-7-9 rule”
- The upper border of liver dullness is defined by:
- 5th intercostal space in the midclavicular line
- 7th intercostal space in the midaxillary line
- 9th intercostal space in the scapular line

➡️ If present in 4th space – Amoebic abscess of liver
➡️ If present in 6th space –
- Pneumonia
- Cirrhosis (Terminal)
- Air in peritoneal cavity
➡️ Pneumothorax – shifting dullness (both air + fluid)
C. Auscultation:
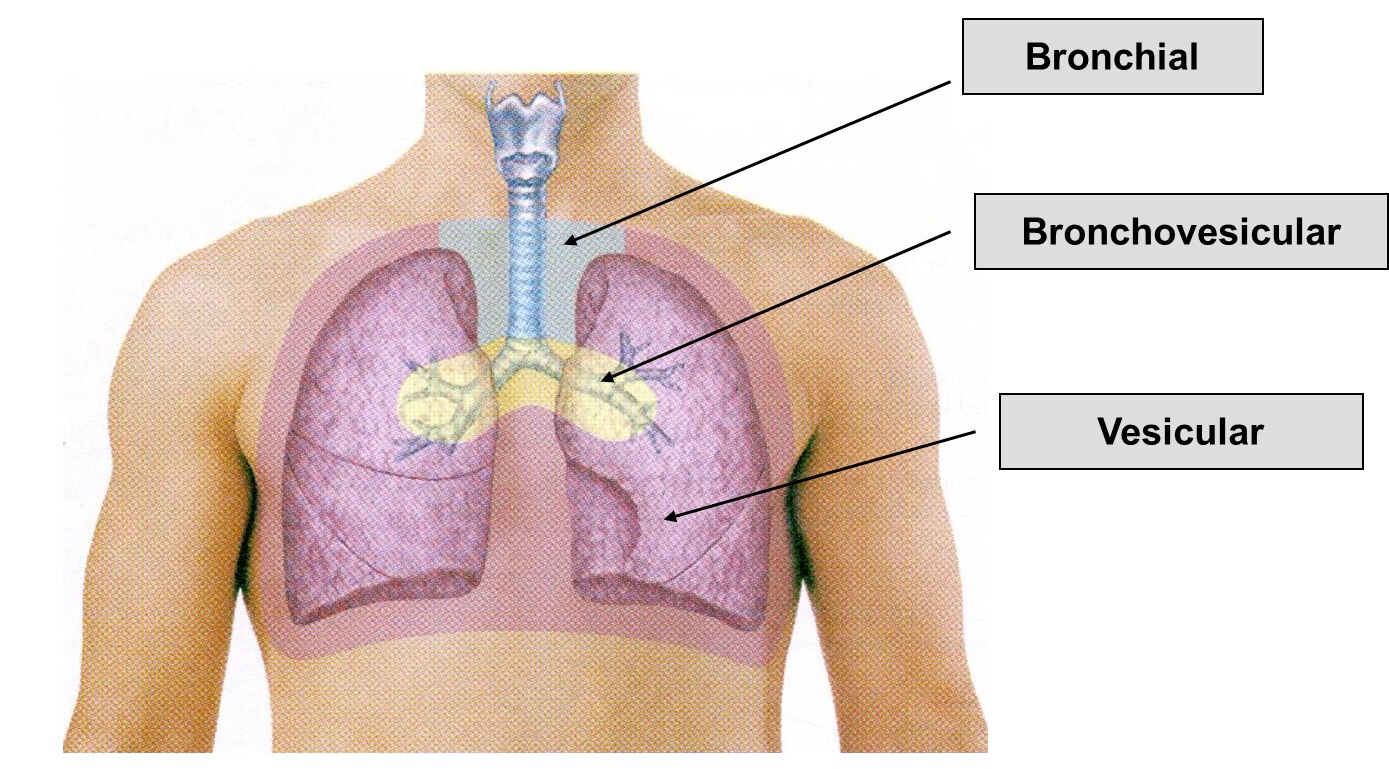
Image©️pinterest
1) Vesicular breath sounds:
➡️ Vesicular breath sounds are heard across the lung surface. They are lower-pitched, rustling sounds with higher intensity during inspiration. During expiration, sound intensity can quickly fade. Inspiration is normally 2-3 times the length of expiration.
➡️ Various Types of Vesicular Breath Sound:
- Exaggerated or puerile vesicular breath sounds: It is normal vescicular breathing with relatively greater clarity. It is common in children and thin built individual.
- Diminished or absent breath sounds: Various causes are shallow breathing, airway obstruction, bulla, hyperinflation, pneumothorax, pleural effusion or thickening, and obesity.
- Normal vesicular breath sound with prolonged expiration: It can occur in obstructive airway diseases like asthma and chronic bronchitis.
2) Bronchial breath sounds:
➡️ The bronchial breath sounds over the trachea has a higher pitch, louder, Expiratory phase is longer than inspiratory phase and there is a pause between inspiration and expiration.
➡️ It is normally heard anteriorly over the manubrium and posteriorly between the C7 and T3 vertebrae.
➡️ The vesicular breathing is heard over the thorax, lower pitched and softer than bronchial breathing.
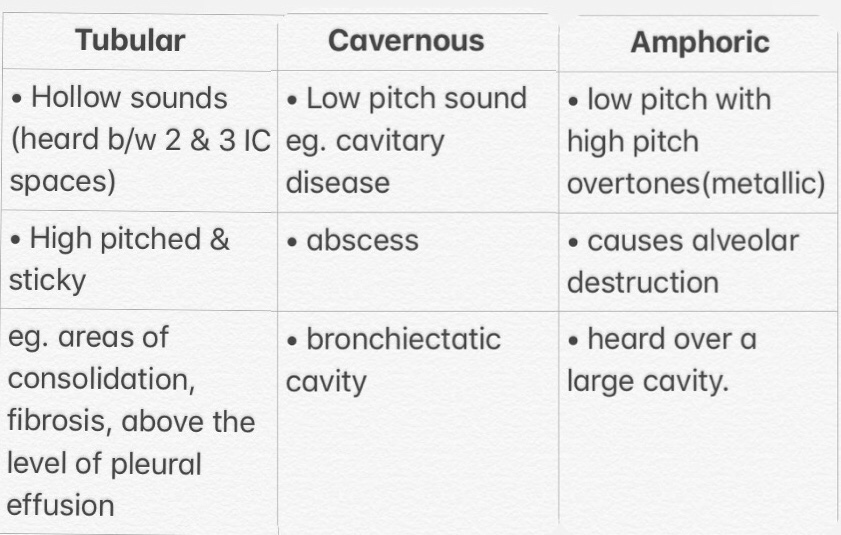
Bronchial sound types👇🏻
3) Bronchovesicular breath sounds:
➡️ It is intermediate between bronchial and vescicular breathing. It has intermediate intensity and pitch with same duration of inspiratory and expiratory phase. It is normally heard anteriorly over 1st and 2nd intercostal spaces and between scapulae posteriorly.
▪️Foreign Sounds:

References:
CHEST XRAY INTERPRETATION
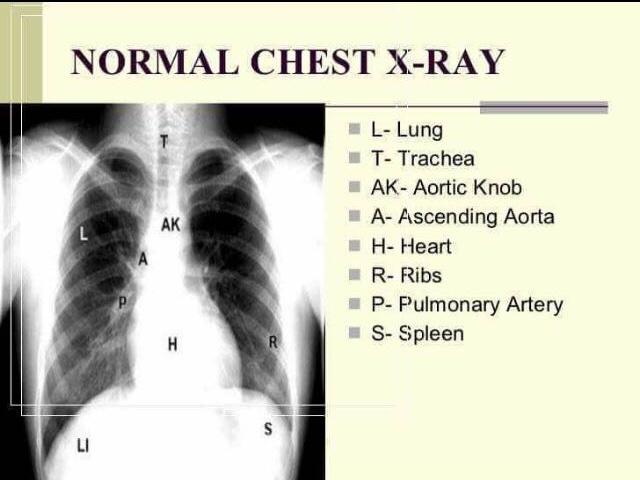
1) NORMAL CHEST XRAY
©️firstaidadvice 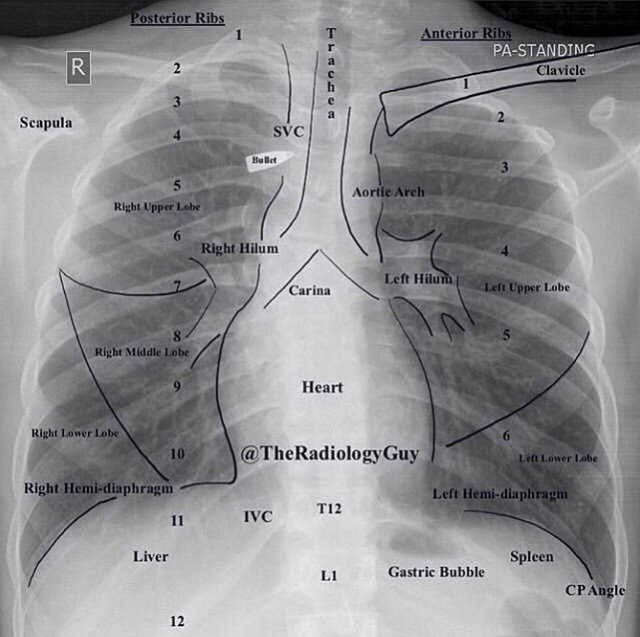
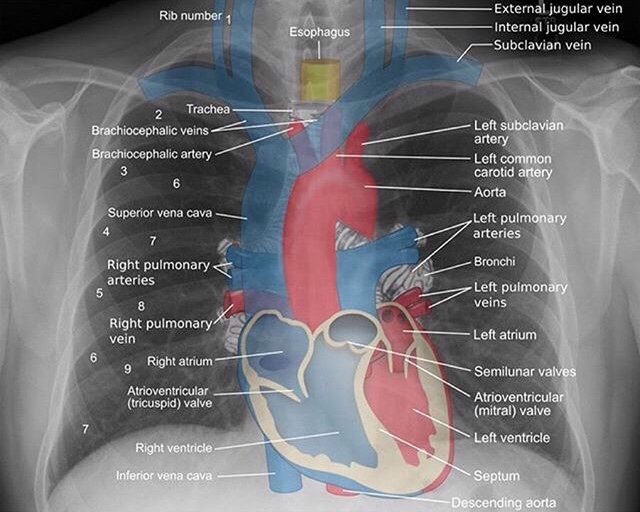
•THE CHEST X-RAY•
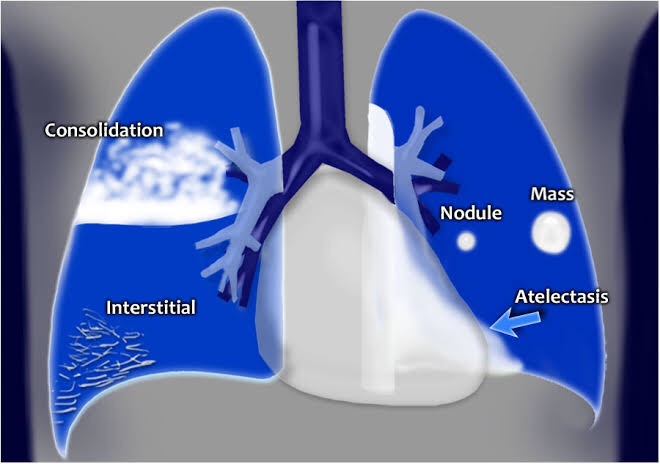
Airway: The trachea is located in the midline. Inspect the trachea and right and left main bronchi. If the trachea is pushed to the left or right look for a cause. Either mass effect pushing the trachea or volume loss (atelectasis) pulling on it.
Breathing: The lobes of the lungs. 3 on the right (upper, middle, lower) and two on the left (upper and lower). Look for consolidation, nodules, masses. Things replacing normal aerated lung (black) will show up as white.
Cardiac: look at the heart size (should be less than 50% of the diameter of the chest). Make sure the borders are clear and sharp. The right atrium makes up the right heart border and the left ventricle makes up the left heart border on the chest X-ray. If the border is obscured, think pneumonia or mass.
Diaphragm: should be well defined to the costophrenic angle. Becomes obscured by lower lobe pneumonia and pleural effusions. Always look for free air under the diaphragm.
Everything else:
- Bones – look for fractures and destructive lesions
- Hilar contours – look for enlargement caused by lymphadenopathy or masses
- Vascular structures – enlarged pulmonary arteries and aortic aneurysms.
Page 1 of 14
2) PLEURAL EFFUSION
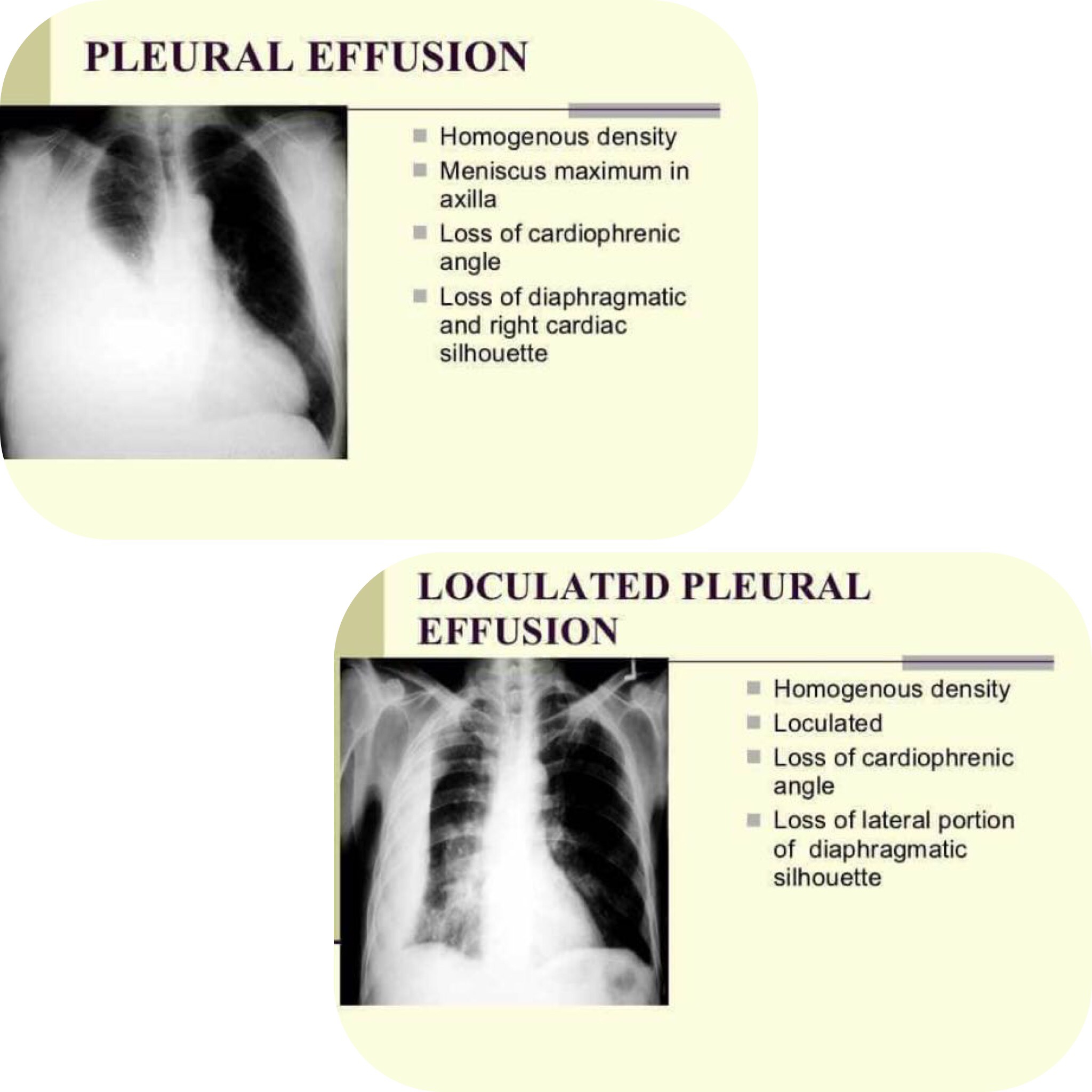
⬇️ Vertical Dimension
1) Mediastinal shift to opposite side
2) Blunting of costophrenic angle
3) Homogenous opacity (Presence of fluid)
4) Ellis S-shaped curve (Concave border)
▪️Causes:
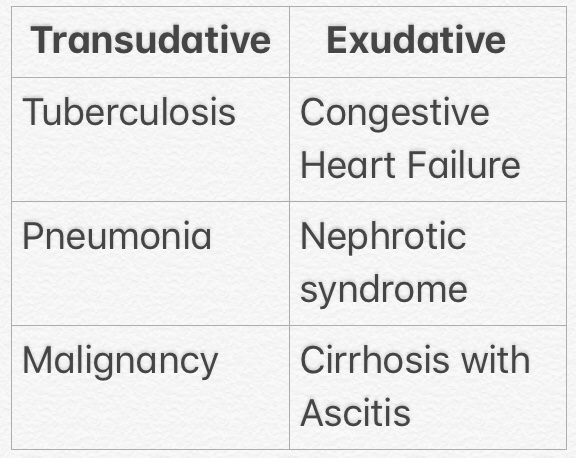
▪️Treatment:
➡️ Both treatment and prognosis are completely dependent on the underlying cause:
- an infected effusion should be drained with an intercostal drain
- a large effusion secondary to heart failure or in a patient with cirrhosis may respond to diuretics
- an effusion secondary to malignancy may require pleurodesis following drainage
Page 2 of 14
Read More »EXAMINATION OF ABDOMEN – PART 2

Examining the abdomen in quadrants remembering the organs that occupy the quadrants will give an indication of the problem for example:
👉🏼Pain in all quadrants with associated vomiting and diarrhea may indicate gastroenteritis.
👉🏼Colicky pain in all quadrants may indicate an obstruction of the bowel.
👉🏼Pain from appendicitis is usually in the right lower quadrant.
👉🏼Pain from a gastric ulcer is usually in the top 2 quadrants more on the left than the right.
👉🏼Pain from a ruptured ectopic pregnancy will be in the lower quadrant on the affected side.
👉🏼Pain in the lower quadrants together with increased frequency of passing urine and pain when passing urine indicates an infection in the urinary tract (UTI)
Contd…Page 2 (Abdominal Quadrants)👇🏻
Read More »MOA OF LOCAL ANAESTHESIA

source – don’t remember, had written it a lot time ago
