BY Dr. KRITI NAJA JAIN :-
1. FIBROUS DYSPLASIA :-
Def:- Fibrous dysplasia is an uncommon nonhereditary, developmental anomaly of the bone due to a defect in osteoblastic differentiation and maturation.
HISTOPATHOLOGY:
- Microscopic finding of fibrous dysplasia show irregularly shaped trabeculae of immature (woven) bone in a cellular, loosely arranged fibrous stroma.
- The bone trabeculae are not connected to each other . They often assume curvilinear shapes.
- which have been likened to CHINESE script writing.
- The bone trabeculae are considered to arise by metaplasia and are not surrounded by plum appositional osteoblasta.


2. PAGET’S DISEASE (OSTEITIS DEFORMANS):-
Def:- Paget’s disease of bone is a condition characterized by abnormal and anarchic resorption and deposition of bone, resulting in distortion and weakening of the
affected bones.
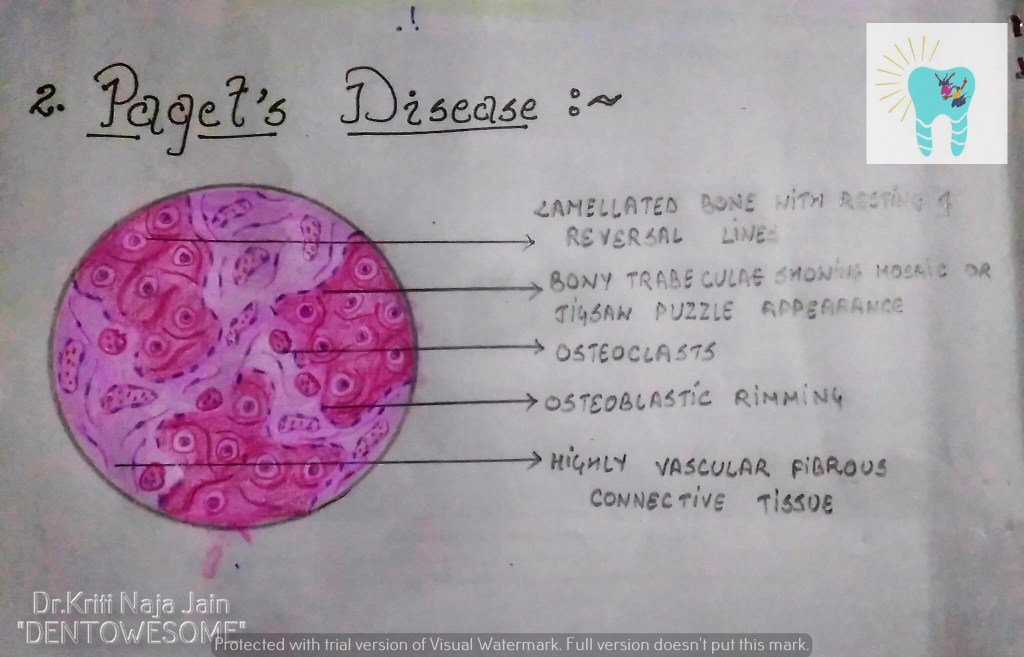
HISTOPATHOLOGY:-
- Microscopic examination shows an apparent uncontrolled alternating resorption and formation of bone.
- in the active resorption stages, numerous osteoclasts surround bone trabeculae and show evidence of resorption activity.
- Simultaneously ,osteoclastic activity is seen with formation of osteoid rims around bone trabeculae .
- A highly vascular fibrous C.T. replaces the marrow .
- A characteristic microscopic feature is the presence of basophilic reversal lines in the bone.
- These lines indicate the junction between alternating resorptive and formative phase of the bone and result in a ” JIGSAW PUZZLE” or “MOSAIC” appearance of the bone.
- In the less active phases ,large masses of dense bone showing prominent reversal lines are present.

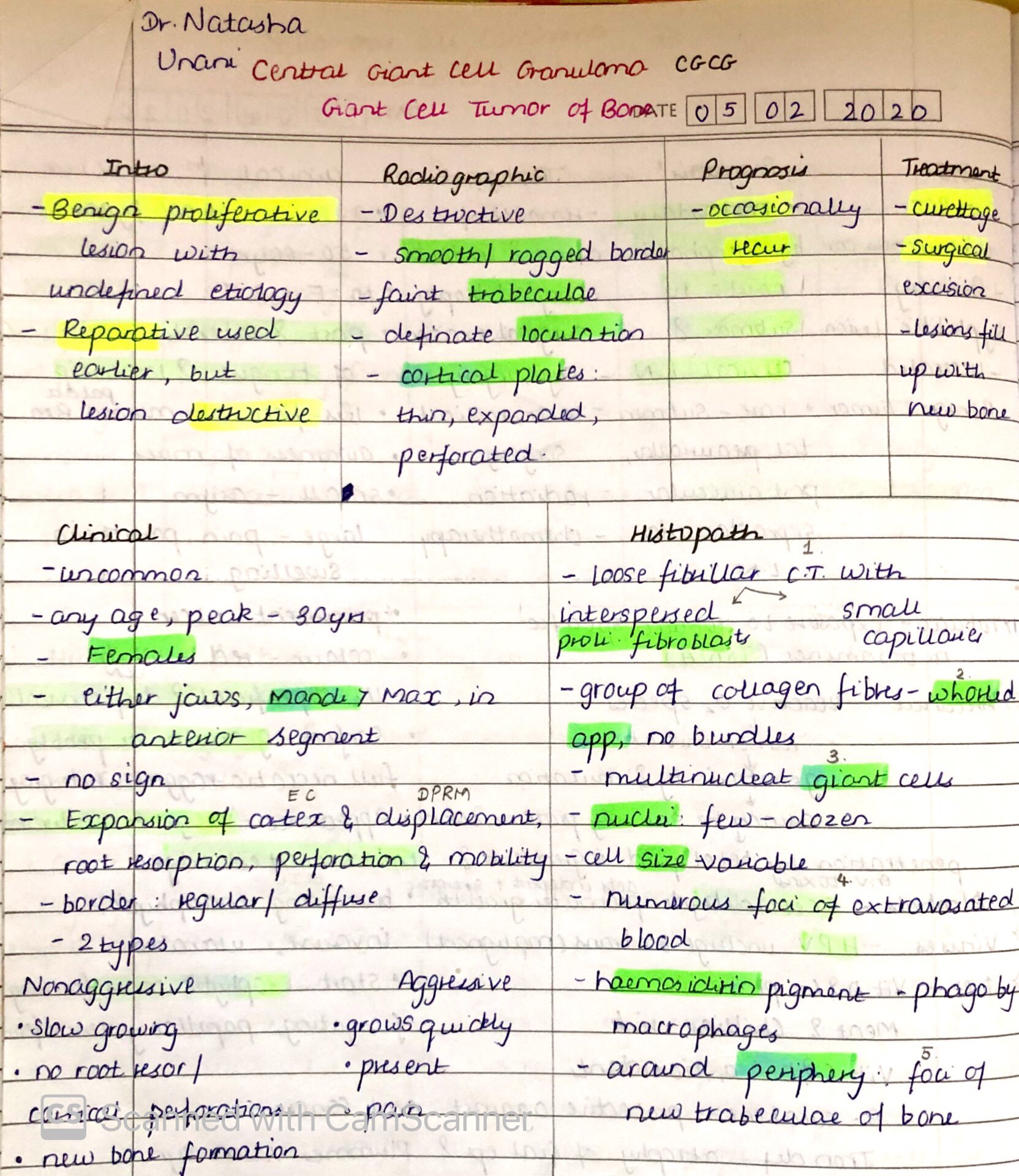
3. CENTRAL GAINT CELL GRANULOMA(GIANT CELL LESION; GIANT CELL TUMOR):-
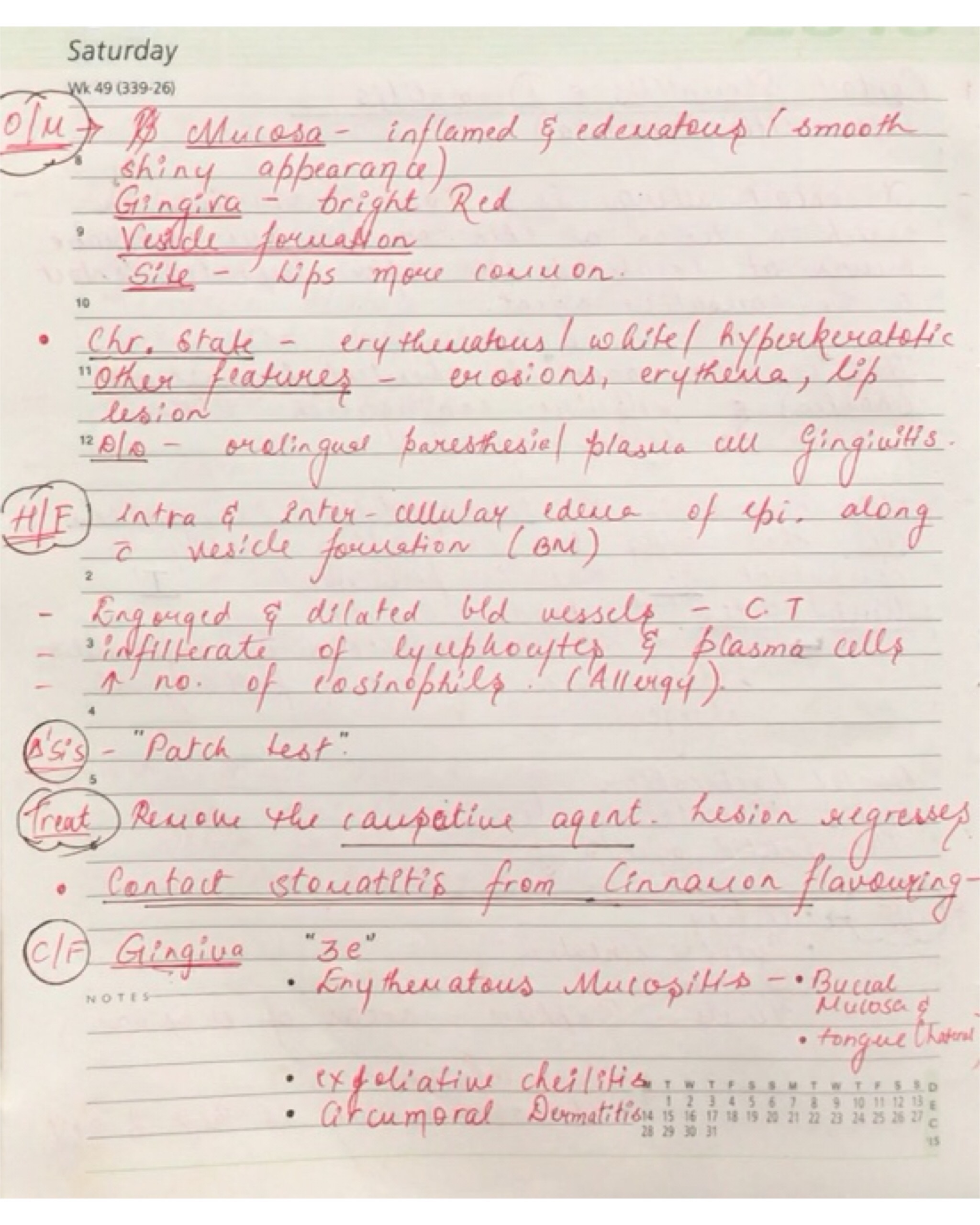
Def :- Central giant cell granuloma (CGCG) is an uncommon, benign and proliferative lesion whose aetiology is not defined. Central giant cell granuloma is a relatively common benign intraosseous destructive giant cell lesion, which often affects the anterior part of the jawbone. By seeing clinical and radiographically , CGCG is divided into two types:-
1. Nonaggressive lesions make up most cases, exhibit few or no symptoms, demonstrate slow growth, and do not show cortical perforation or root resorption of teeth involved in the lesion.
2. Aggressive lesions are characterized by pain, rapid growth, cortical perforation, and root resorption. They show a marked tendency to recur after treatment, compared with the nonaggressive types.
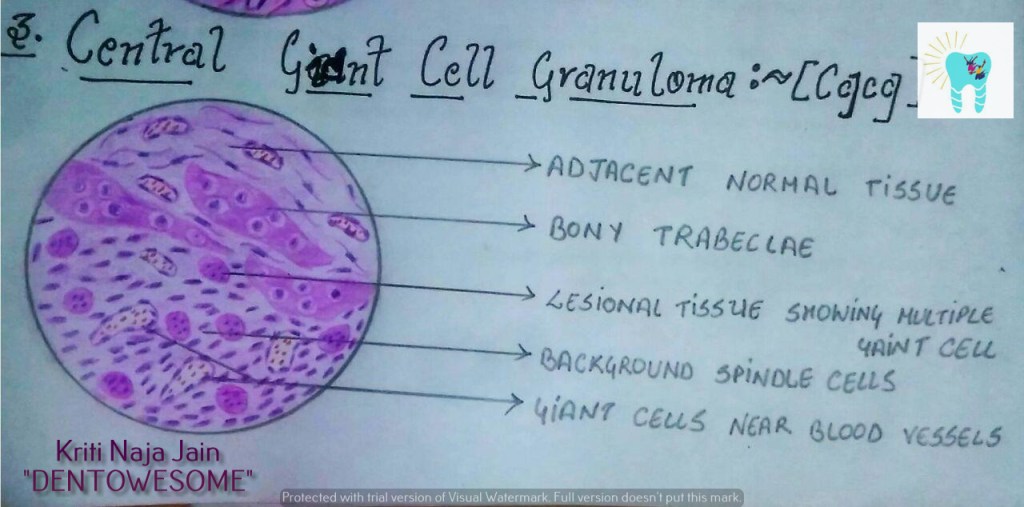
HISTOPATHOLOGY:-
- Lesional tissue is composed of highly cellular connective tissue stroma with numerous spindle shaped cells.
- Multinucleated giant cells are distributed in this C.T.
- Mesenchymal cells
- Gaint cells are large with many nuclei upto 20 or more.
- Gaint cells are usually aggregated close to the blood vessels.

REFERENCE:-
1.Maji Jose 2nd edition