• It is the surgical resection of the apex of the root.
• It is the procedure done in case of root canal treatment failure.
• If an infection does not subside even after root canal treatment,it may concern enquire a surgical procedure.
• In this procedure, the apical region of root is visualised by reflecting a flap and performing an osteotomy.
INDICATIONS :
• Aberrant Anatomy: Dilaceration of root apex do not allow endodontic restoration of apex.
• Obliteration of apex by secondary dentin.
• Iatrogenic repair: A broken endodontic file which cannot be retrieved by conventional means.
• Apex perforation.
• Improper apical seal which cannot be removed.
• Increased drainage of pus from root canal will not allow adequate apical seal.
• Open apex.
• Non healing periapical granuloma.
• Fracture of apical third of root.
• Periapical cyst/granuloma.
CONTRAINDICATIONS:
- Local Contraindications:
• Poor periodontal status of tooth.
• Grossly decayed tooth.
• Inadequate tooth length.
• Acute infection.
• Traumatic occlusion.
• Uncooperative patients.
• Close proximity of root apex to vital anatomic structures such as Maxillary antrum & Nasal floor. - Systemic Contraindications:
• Poor medical status of diabetes,Bleeding disorders.etc
STEPS IN ENDODONTIC SURGERY:
- Cleaning of the area involved with antiseptic solutions.
- Local anaesthesia.
- Design of mucoperiosteal flap & reflection of flap.
- Bone removal for access to root tip.
- Root tip resection & curettage.
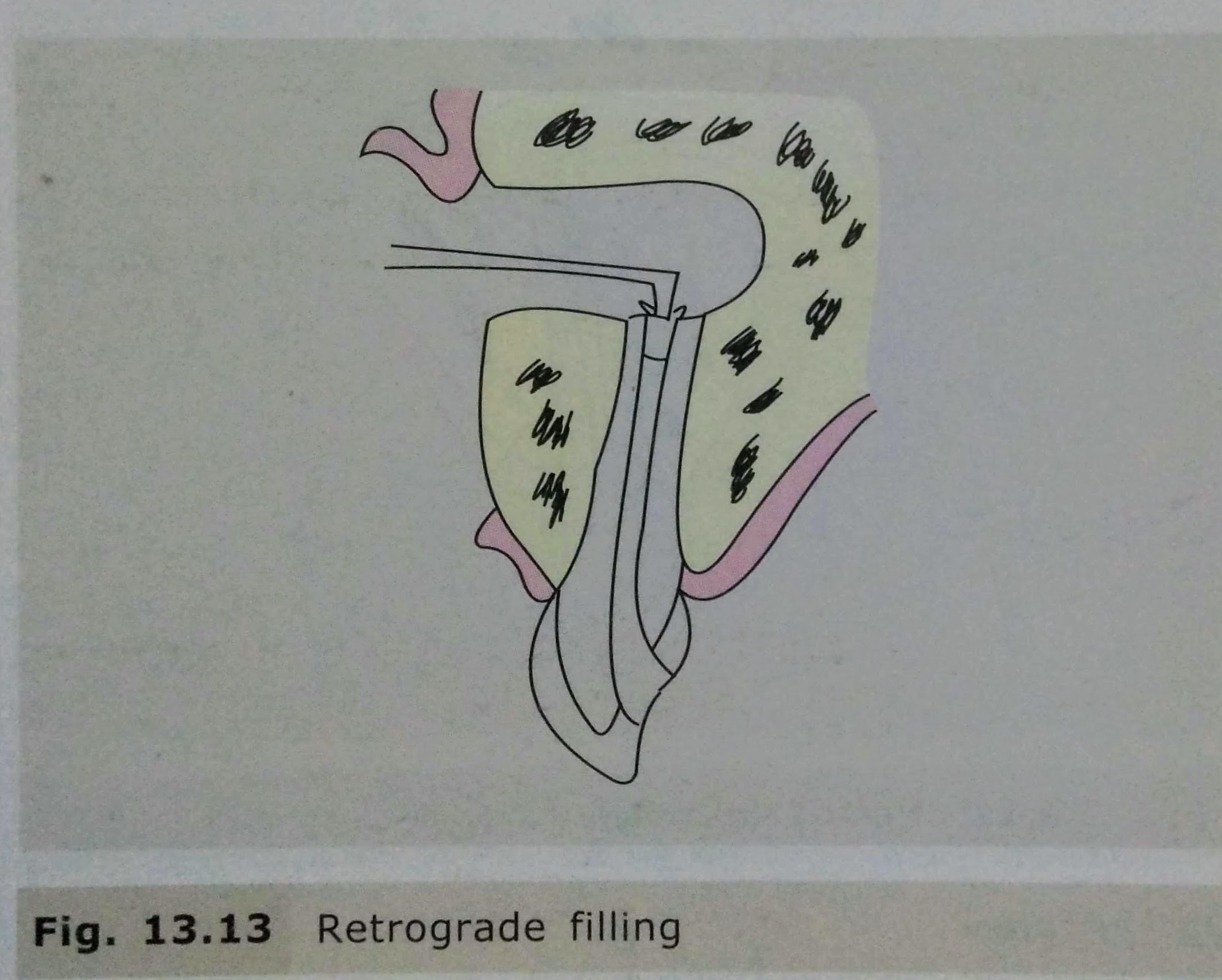
- Retro preparation & retrograde filling.
- Suturing & Follow up.



COMPLICATIONS:
• Mobility of tooth/adjacent tooth.
• Haemorrhage.
• Nasal perforation.
• Oroantral Fistula.
• Mental Nerve Damage.
• Inferior Alveolar Nerve damage.
REFERENCES:
• Textbook of Oral & Maxillofacial Surgery, Chitra Chakravarthy (2nd Edition)
• DentaGama.com