I Kriti Jain, an undergraduate student, pursuing "Bachelor of Dental Surgery" from Teerthankar Mahaveer Dental College and Research Center, Moradabad, Uttar Pradesh.
I'm privileged to join this wonderful platform where I interact with many beautiful, hardworking, and ambitious souls. The atmosphere is friendly, the ambiance motivating. Students like me are able to make humble contributions by writing articles which means a lot to us.
Dentistry is a combination of art and science which I realized after entering the field. This is different from the general stereotype about dentistry in our society. I want to change this perspective and show the world that dentists are as important as other doctors.
Let's together make dentistry great again :)
Careful examination of the oral cavity may reveal findings indicative of an underlying systemic condition, and allow for early diagnosis and treatment. Examination should include evaluation for mucosal changes, periodontal inflammation and bleeding, and general condition of the teeth.
I.GIT Diseases • Gastrointestinal diseases refer to diseases involving the gastrointestinal tract, namely the esophagus, stomach, small intestine, large intestine and rectum, and the accessory organs of digestions, the liver, gallbladder, and pancreas.
• Crohn’s disease, also known as Crohn syndrome and regional enteritis, is a type of inflammatory bowel disease (IBD). • Ulcerative colitis is a form of inflammatory bowel disease (IBD) that causes inflammation and ulcers in the colon. • Gastroesophageal reflux is a chronic symptom of mucosal damage caused by stomach acid coming up from the stomach into the esophagus. • Chronic liver disease in the clinical context is a disease process of the liver that involves a process of progressive destruction and regeneration of the liver parenchyma leading to fibrosis and cirrhosis.
1. Crohn disease:– – diffuse labial, gingival or mucosal swelling – „cobblestoning“ of buccal mucosa and gingiva – aphtous ulcers – mucosal tags – angular cheilitis – oral granulomas
2.Ulcerative colitis:- – oral signs are present in periods of exacerbation of disease – aphtous ulceration or superficial hemorrhagic ulcers – angular stomatitis – pyostomatitis vegetans, pyostomatitis gangrenosum.
3.Gastroesophageal reflux:- – reduction of the pH of the oral cavity below 5,5
– enamel damage – damage of the dentin – higher sensitivity (to temperature..), caries
Name suggested by Willis. Most common neoplasm of salivary gland tumor. Benign neoplasm- consisting of cells exhibiting the ability to differentiate to epithelial (ductal and nonductal) cells and mesenchymal (chondroid, myxoid, osseous) cells. Other names:
Branchioma,
enclavoma,
teratoma,
cyindroma,
myxochondrocarcinoma.
Salivary gland tumor origin: EPITHELIAL
Shows cytogenic abnormalities in chomosomes- 12q13-15. Putative pleomorphic adenoma gene(PLAG1) has been mapped to chromosomes 8q12
Histogenesis:-
Currently, numerous theories centre around the myoepithelial cell and the reserve cell in the intercalated duct.
Ultrastructural studies have confirmed the presence of both ductal and myoepithelial cells in pleomorphic adenomas.
It follows that possibly either or both may play active roles in the histogenesis of the tumour.
Hubner and his associates:- have postulated that the myoepithelial cell is responsible for the morphological diversity of the tumour, including the production of the fibrous, mucinous, chondroid and osseous areas.
Regezi and Batsakis:- postulated that the intercalated duct reserve cell can differentiate into ductal and myoepithelial cells, and the latter, in turn, can undergo mesenchymal metaplasia, since they inherently have smooth muscle-like properties. Further differentiation into other mesenchymal cells then can occur.
Batsakis:- has discussed salivary gland tumourigenesis, and while still implicating the intercalated duct reserve cell as the histogenetical precursor of the pleomorphic adenoma, stated that the role of the myoepithelial cell is still uncertain and that it may be either an active or a passive participant histogenetically.
Finally, Dardick and his associates have questioned the role of both ductal reserve and myoepithelial cells. They stated that a neoplastically altered epithelial cell with the potential for multidirectional differentiation might be histogenetically responsible for pleomorphic adenoma.
CLINICAL FEATURES:-
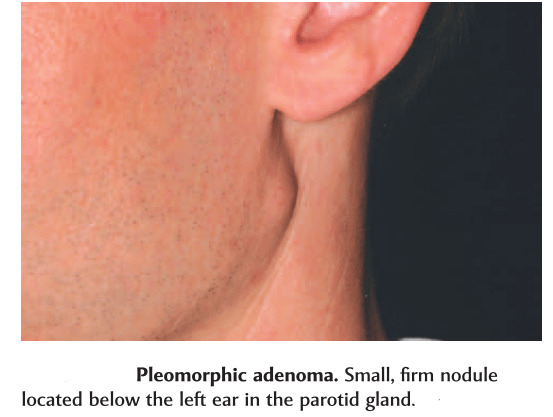
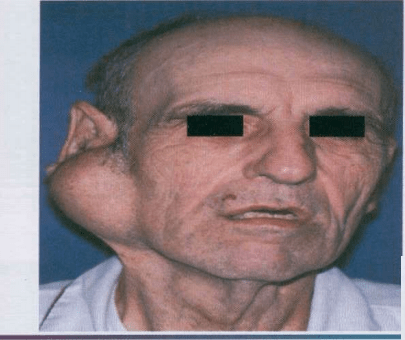
Most common tumor. Rate of occurance: 60-70%- parotid glands 40-60%- submandibular glands 40-70%- minor salivary glands seldomly- sublingual glands Age: 30-50 years Sex: female> male – 3:1 – 4:1 In parotid- presents in the lower lobe of the superior lobe as a mass over the angle of the mandible, below and infront of the ear.
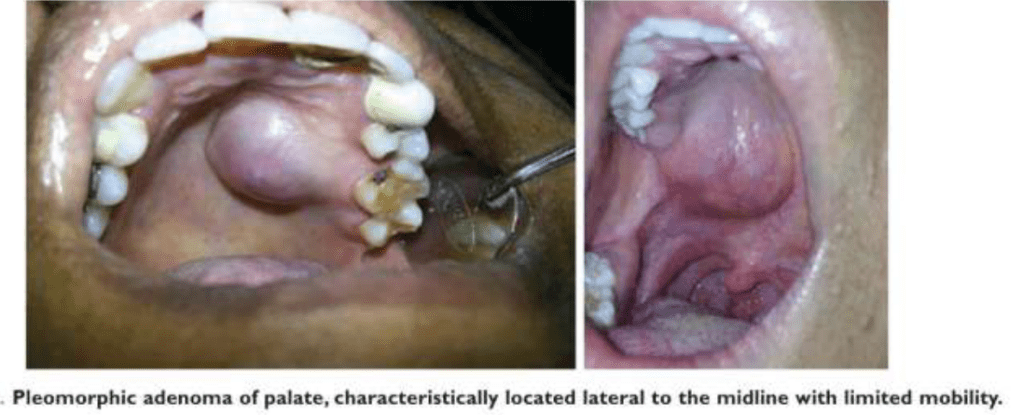
Clinical presentation: painless, slow growing, firm mass, initially small in size and begins to increase in size. Initially movable but with continued growth become more nodular and less movable. Recurrent tumor- multinodular, fixed on palpation. Palate – intraorally common site. Seldom ulcerated- unless secondarily traumatized.
Slowly growing tumor of The parotid gland.
HISTOPATHOLOGY:-
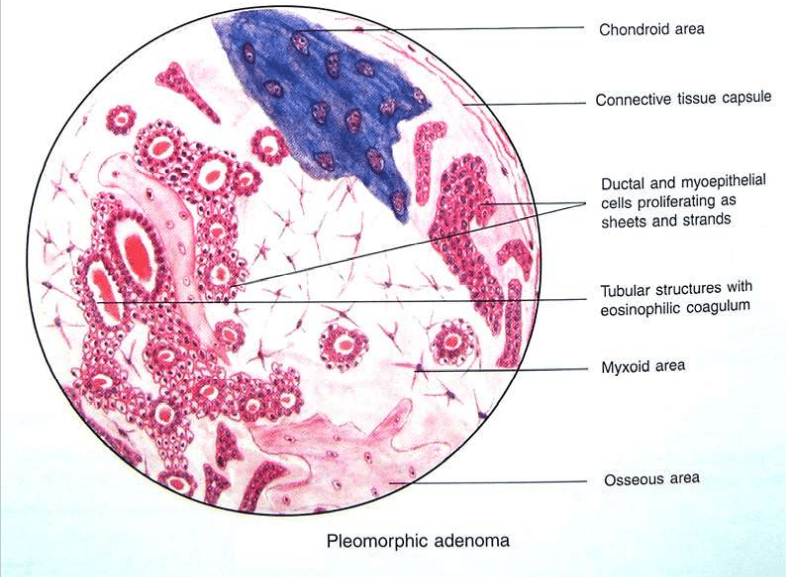
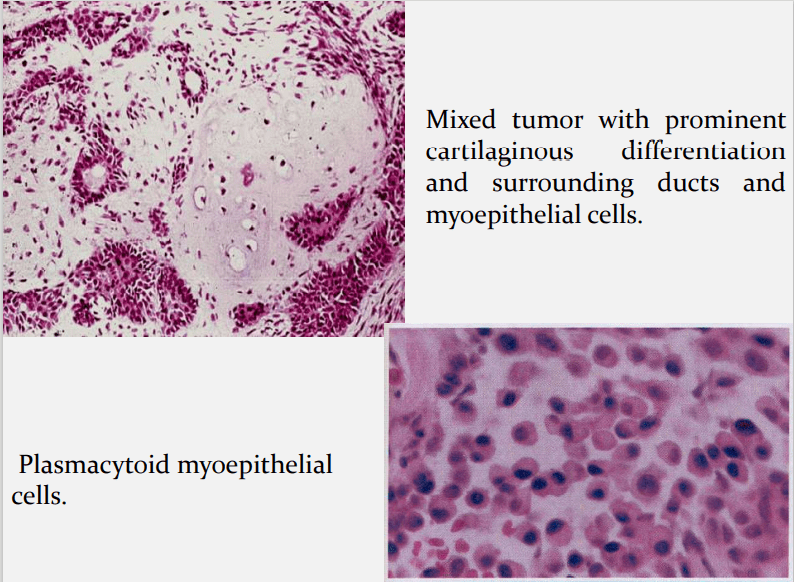
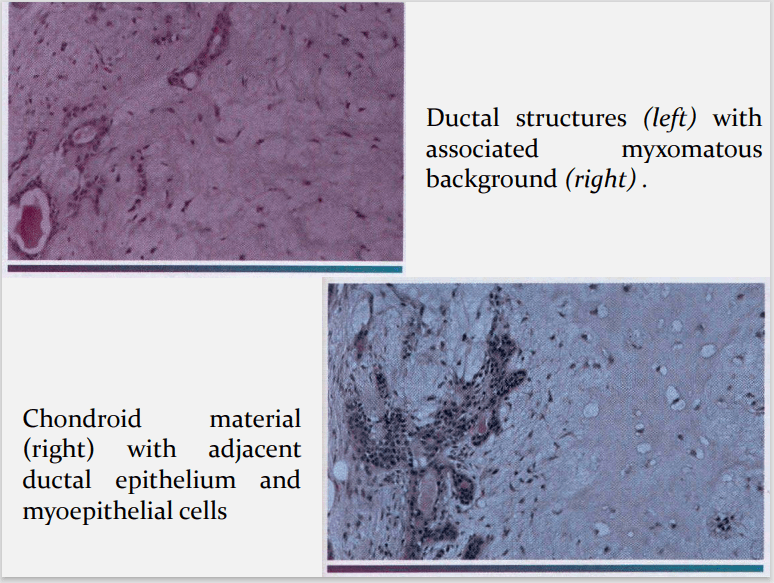
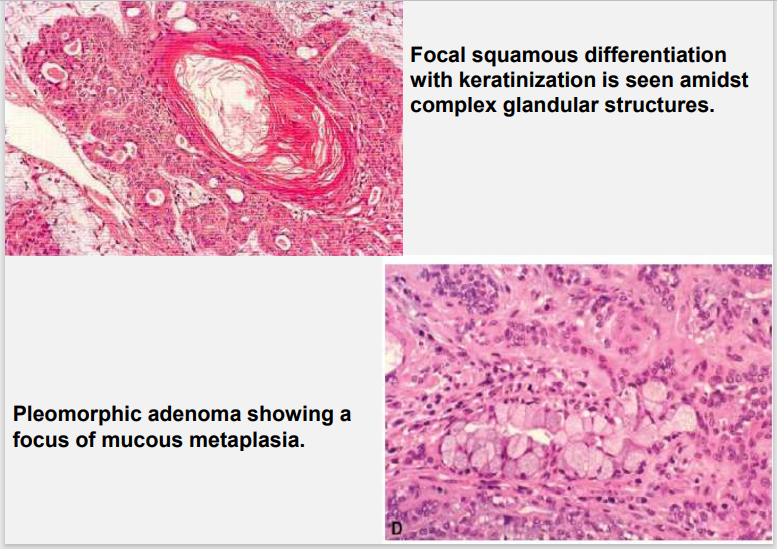
HALLMARK: Morphologic Diversity. Charecterized by- Variable, Diverse, Structural & histologic patterns. It demonstrate glandular epithelium and mesenchyme like tissue and the proportion of each component varies widely. Typically a well-circumscribed encapsulated tumor The epithelium often forms ducts and cystic structures or may occur as islands or sheets of cells , anastomosing cords and foci of Keratinizing squamous cells and spindle cells .
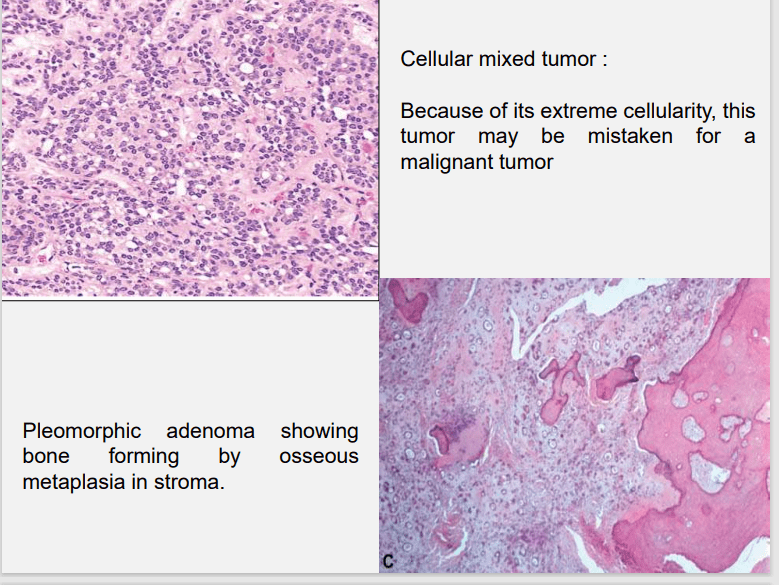
Foote and Frazell (1954) categorized PA into: a) Primarilly myxoid (36%) b) Myxoid and cellular component in equal proportions (30%) c) Predominantly cellular (22%) d) Extremely cellular (12%)
Myoepithelial cells are major component of PA. Have variable morphology- sometimes appearing as angular or spindled, some with eccentric nucleus resembling plasma cells. Are responsible for characteristic mesenchyme like changes. Vacuolar degeneration of myoepithelial cells can produce a chondroid appearance. the stroma exhibits areas of an eosinophilic hyalinized change, fat or osteoid also is seen.
Surgical excision Superficial parotidectomy with preservation of the facial nerve Local enucleation should be avoided – resulting in seeding of the tumor bed. Deep lobe of the parotid- total parotidectomy is usually necessary also with preservation of the facial nerve.
Submandibular tumors – Total removal of the gland with the tumor. Malignant degeneration is a potential complication, resulting in a carcinoma ex pleomorphic adenoma. The risk of malignant transformation is probably small, but it may occur in as many as 5% of all cases.
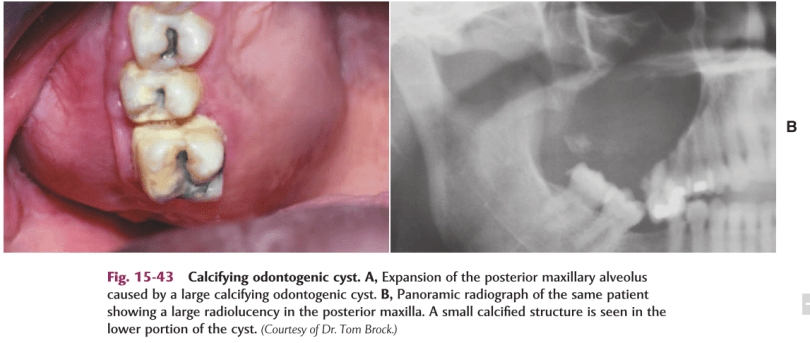
DEF:-Calcifying odontogenic cyst (COC), previously known as Gorlin cyst, is a rare, well-circumscribed, solid or cystic lesion derived from odontogenic epithelium that resembles follicular ameloblastoma but contains ‘ghost cells’ and spherical calcifications.
It Has many features of odontogenic tumor, therefore it is placed in the category of tumors in the latest WHO classification of odontogenic cysts and tumors.
In the latest WHO publication on odontogenic tumours (Prætorius and Ledesma-Montes, 2005) it was classified as a benign odontogenic tumour and was renamed calcifying cystic odontogenic tumour (CCOT).
CLINICALFEATURES:-
Age : Wide range, peak in 2nd decade.
Sex : Equal.
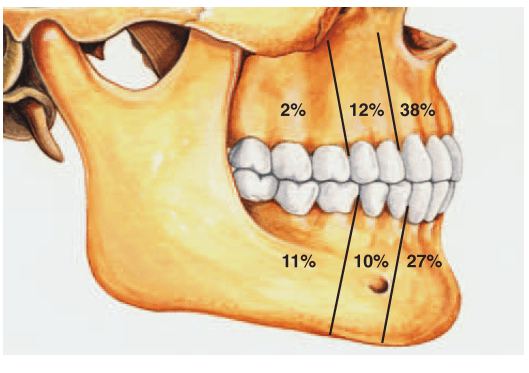
Site : Anterior segment of both jaws
Calcifying odontogenic cysts that are associated with odontomas tend to occur in younger patients, with a mean age of 17 years.
PATHOGENESIS:-
COC is a unicystic process and develops from the reduced dental epithelium or remnants of dental lamina.
The cyst lining has the potential to induce formation of dentinoid or even odontoma in adjacent CT wall.
CLASSIFICATION OF THE ODONTOGENIC GHOST CELLLESIONS:-
Group 1 : ‘Simple’ cysts Calcifying odontogenic cyst (COC)
Group 2 : Cysts associated with odontogenic hamartomas or benign neoplasms: calcifying cystic odontogenic tumours (CCOT).
Group 3 : Solid benign odontogenic neoplasms with similar cell morphology to that in the COC, and with dentinoid Formation
.Group 4 : Malignant odontogenic neoplasms with features similar to those of the dentinogenic ghost cell tumour Ghost cell odontogenic carcinoma.
SIGNS &SYMPTOMS:-
Swelling is the commonest complaint, seldom associated with pain.
Intraosseous lesions can cause hard bony expansion and resulting facial asymmetry.
Displacement of teeth can also occur.
RADIOLOGICALFEATURES:-
Intraosseous lesions produce well defined lucency which is usually unilocular.
Irregular calcified masses of varying sizes may be seen within the lucency.
Displacement of root/roots with or without root resorption and expansion of cortical plates also seen.
*Radiograph of a calcifying odontogenic cyst with well-demarcated margins extending from the right to the left premolar regions of the mandible. Numerous calcifications are present, some suggestive of small denticles.
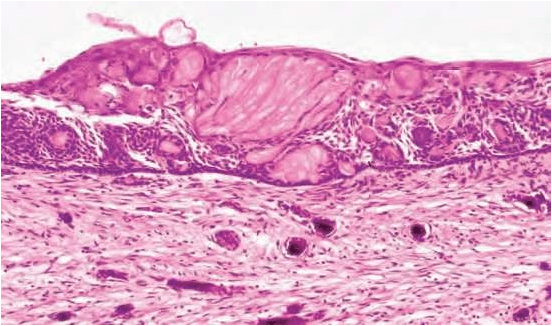
HISTOLOGICALFEATURES:-
Lining is usually thin about 6 – 8 cell thick, may be thickened in other areas.
Lining shows characteristic odontogenic features with reversely polarized basal cell layer.
TYPICALLY – GHOST CELLS may be seen in thicker areas of lining.
Ghost cells are enlarged, ballooned, ovoid, eosinophilic cells with well
defined cell boundaries.
5.Some times many cells may fuse.
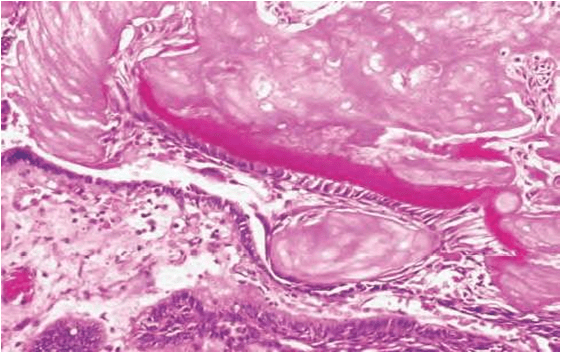
6.They represent abnormal keratinization and frequently calcify.
7.Tubular dentinoid and even complex odontome may be found in connective tissue wall close to epithelial lining.
Histological features of a calcifying odontogenic cyst with clusters of fusiform ghost cells and focal calcifications, lying in a stratified squamous epithelium.In this calcifying odontogenic cyst, there are sheets of ghost cells and a focal area in which there has been induction of a strip of dysplastic dentine (dentinoid).
DIFFERENTIALDIAGNOSIS:-
Based on radiographic appearance, following lesions must be included in the provisional diagnosis –
Def:- Fibrous dysplasia is an uncommon nonhereditary, developmental anomaly of the bone due to a defect in osteoblastic differentiation and maturation.
HISTOPATHOLOGY:
Microscopic finding of fibrous dysplasia show irregularly shaped trabeculae of immature (woven) bone in a cellular, loosely arranged fibrous stroma.
The bone trabeculae are not connected to each other . They often assume curvilinear shapes.
which have been likened to CHINESE script writing.
The bone trabeculae are considered to arise by metaplasia and are not surrounded by plum appositional osteoblasta.
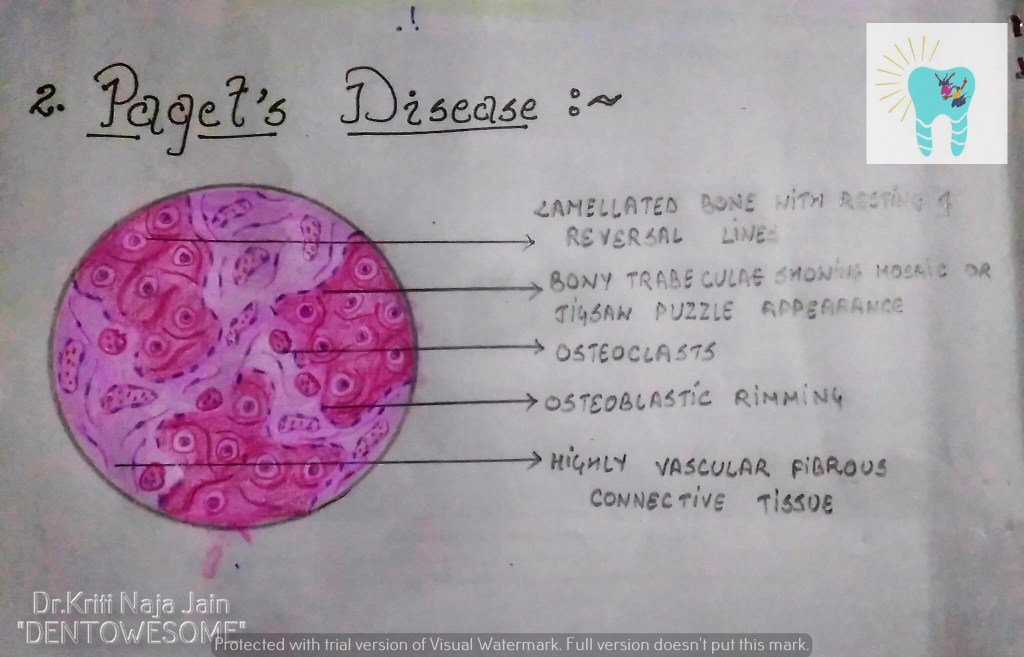
2. PAGET’S DISEASE (OSTEITIS DEFORMANS):-
Def:- Paget’s disease of bone is a condition characterized by abnormal and anarchic resorption and deposition of bone, resulting in distortion and weakening of the affected bones.
HISTOPATHOLOGY:-
Microscopic examination shows an apparent uncontrolled alternating resorption and formation of bone.
in the active resorption stages, numerous osteoclasts surround bone trabeculae and show evidence of resorption activity.
Simultaneously ,osteoclastic activity is seen with formation of osteoid rims around bone trabeculae .
A highly vascular fibrous C.T. replaces the marrow .
A characteristic microscopic feature is the presence of basophilic reversal lines in the bone.
These lines indicate the junction between alternating resorptive and formative phase of the bone and result in a ” JIGSAW PUZZLE” or “MOSAIC” appearance of the bone.
In the less active phases ,large masses of dense bone showing prominent reversal lines are present.
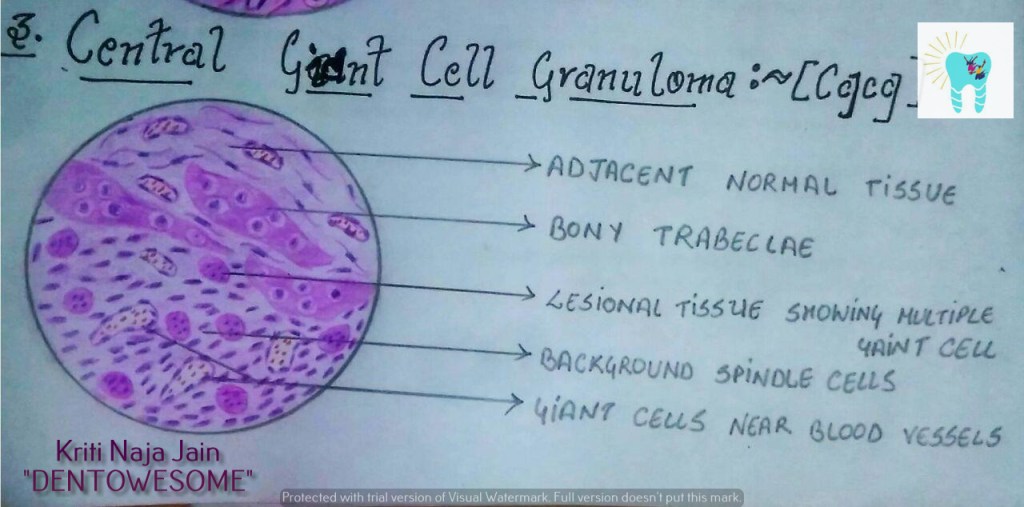
3. CENTRAL GAINT CELL GRANULOMA(GIANT CELL LESION; GIANT CELL TUMOR):-
Def :- Central giant cell granuloma (CGCG) is an uncommon, benign and proliferative lesion whose aetiology is not defined. Central giant cell granuloma is a relatively common benign intraosseous destructive giant cell lesion, which often affects the anterior part of the jawbone. By seeing clinical and radiographically , CGCG is divided into two types:-
1. Nonaggressive lesions make up most cases, exhibit few or no symptoms, demonstrate slow growth, and do not show cortical perforation or root resorption of teeth involved in the lesion. 2. Aggressive lesions are characterized by pain, rapid growth, cortical perforation, and root resorption. They show a marked tendency to recur after treatment, compared with the nonaggressive types.
HISTOPATHOLOGY:-
Lesional tissue is composed of highly cellular connective tissue stroma with numerous spindle shaped cells.
Multinucleated giant cells are distributed in this C.T.
Mesenchymal cells
Gaint cells are large with many nuclei upto 20 or more.
Gaint cells are usually aggregated close to the blood vessels.
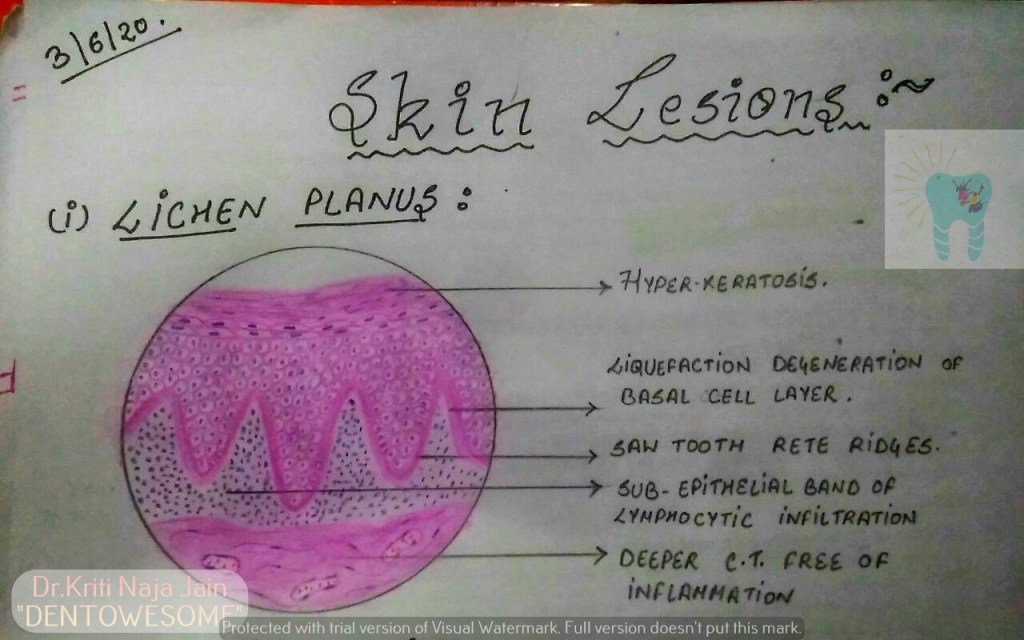
*Lichen planus is a chronic mucocutaneous disorder manifested in a various forms in the oral cavity.
*The most characteristic pattern is” RETICULAR TYPE” with the interlacing white stripe called “WICKHAM’S STRIAE”.
*HISTOPATHOLOGY:-
Histopathology FIRST DESCRIBED BY DUBRENILL 1906
later revised by Shklar in 1972
Hyper orthokeratinisation or hyper parakeratinisation
◦Thickening of granular layer
◦Acanthosis of spinous layer
◦Intercellular oedema in spinous layer
◦“ Saw-tooth” rete pegs
◦Liquefaction necrosis of basal layer- Max Joseph spaces
◦Civatte ( hyaline or cytoid) bodies
◦Juxta epithelial band of inflammatory cells
◦An eosinophilic band may be seen just beneath the basement membrane and represent fibrin covering lamina propria.
2.PEMPHIGUS :-
Pmphigus is a tissue specific autoimmune disease affecting the skin and mucosa. Clinical manifestations is in the from of “vesiculobullous lesions” that rupture to form ulcer and erosions .
*Vesiculobullous lesions develop due to immune mediated acantholysis causing intraepithelial vesicle formation.
*HISTOPATHOLOGY :-
Formation of the vesicle or bullae within the epithelium that often results in a supra-basilar spilt or separation. • Following this suprabasilar spilt in the epithelium, the basal cell layer remains attached to the lamina propria, and it often appears as a row-of-tomb stones. • Loss of intercellular bridges and collection of edema fluid result in acantolysis within the spinus cell layer, which causes disruption of the prickle cells. • As a result of acantholysis, clumps of large hyperchromatic epithelial cells desquamate that are often seen lying free within the vesicular fluid, these desquamated cells are often rounded and smooth in appearance and are known as “Tzanck cells”.
Small number of polymorphonuclear neutrophil (PMN) and lymphocytes may be found within the vesicular fluid, but there is minimum inflammatory cell infiltration in the underlying connective tissue (unlike any other vesiculobullous lesion).
3.PEMPHIGOID :-
Pemphigoid is a vesiculobullous lesions that develop due to an autoimmune reaction directed against some components of basement membrane.
*This results in seperation of epithelium from the connective tissue with sub epithelial vesicles formation .
*Bullous pemphigoid and cicatricial pemphigoid are two different types of pemphigoid lesions.
*HISTOPATHOLOGY:-
The inflammatory infiltrate is typically polymorphous, with an eosinophilic predominance.
Mast cells and basophils may be prominent early in the disease course.
Electron microscope shows basement membrane attached to the connective tissue rather than overlying separated epithelium.