: • Preventive resin restoration (PRR) is a thin, resin coating applied to the chewing surface of molars, premolars and any deep grooves of the teeth. • They are a natural extension of the use of occlusal sealants. • It consists of an enamel sealant with a resin filling. • If caries is present in one area or parts of pits and fissures, that particular area of caries is restored and fissures are protected with sealants. • It integrates the preventive approach of the sealant therapy for caries susceptible pit & fissure with therapeutic restoration incipient caries with composite resin that occur on the same occlusal surface. • They are the conservative answer to conventional extension for prevention” philosophy of Class I amalgam cavity preparation.
Preventive resin restoration(PRR) consists of a thin, resin coating applied to the occlusal surface of molars, premolars and deep grooves. Most decays begin in the deep grooves. Thus, teeth with this condition are difficult to clean and becomes more susceptible to caries. PRR protects the tooth by sealing the deep grooves and creating a smooth, easy to clean surface. By this way, the teeth is protected from decay for several years, provided they are checked for thinning and wear at regular dental check-ups.
Dental caries is due to the imbalance between loss & gain of
minerals from a tooth surface.
The loss of minerals from our teeth occurs from the bacteria from the foods and producing acids, whereas the tooth gains minerals from our saliva and fluoride that is present within our mouth which over a period of time becomes a tooth decay.
Fissure sealants are a preventive treatment that is part of the minimal intervention dentistry approach to dental care.
This approach facilitates prevention and early intervention, in order to prevent or stop the dental caries process before it reaches the ends stage of the disease.
CLASSIFICATION:
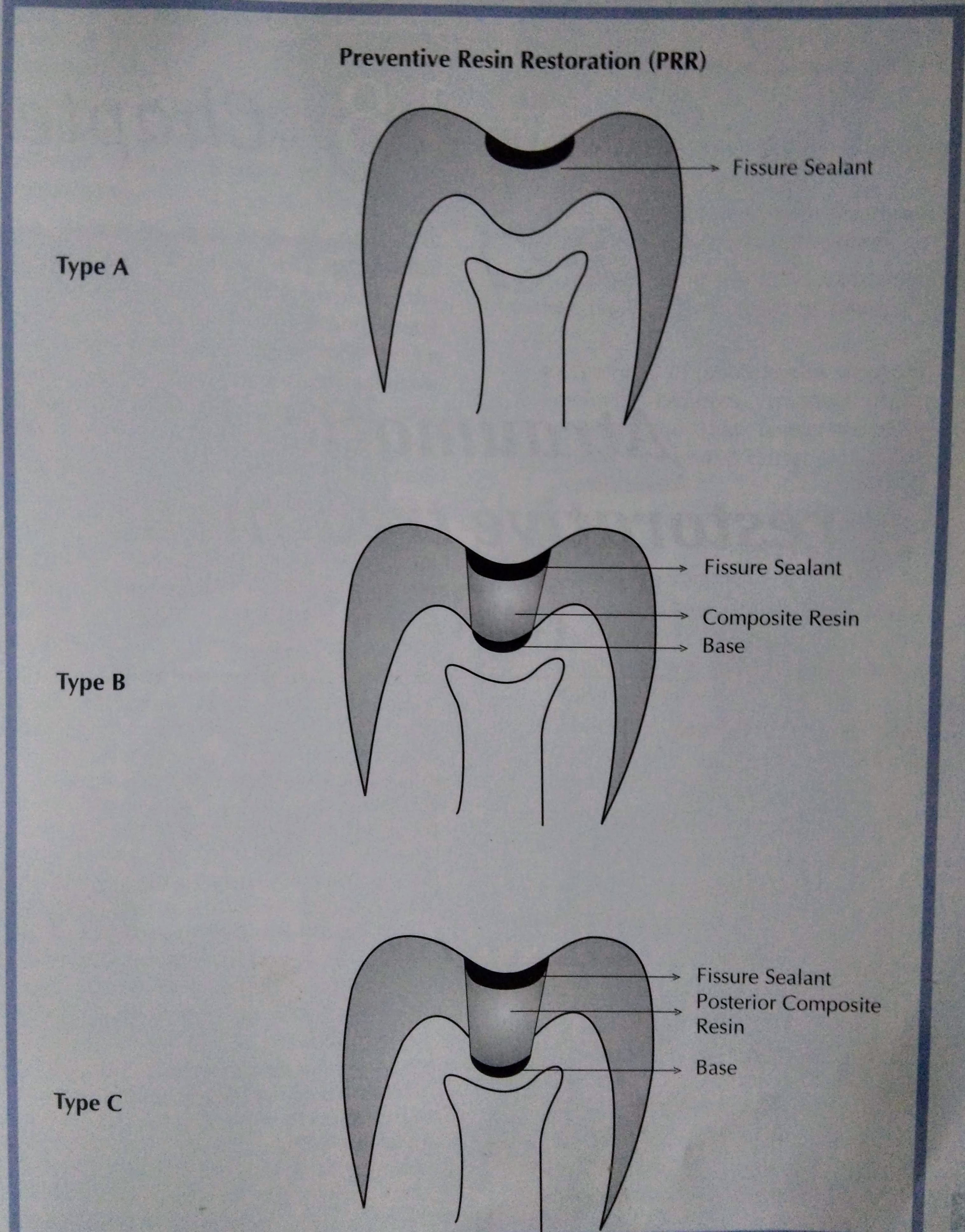
There are three types of preventive resin restoration based on the extent & depth of carious lesion as determined by exploratory preparation.
Simonsen (1978) has classified them:
TYPE A:
• Suspicious pits & fissures where caries removal is limited to enamel • Local anesthesia is not required. • A slow speed 4 or 2 round burs. used to remove decalcified enamel • Sealant is placed
TYPE B:
• Incipient lesion in dentin that is small & confined. • No local anesthesia is needed. • An appropriate base is placed in areas of dentin exposure, composite resin is placed & the remaining pit & fissure are covered with a sealant.
TYPE C: • More extensive dentinal involvement & requires restorations with posterior composite material • Appropriate base is placed over the dentin. • Pits & fissures are covered with sealant. • Local anesthesia is required.
PROCEDURE:
CONCLUSION: • Regular maintenance and sealant addition when necessary is important in long-term caries protection after sealant placement. • Much better effectiveness data will result if sealants are used on teeth with a true predilection to caries. • Better materials and better use of bonding agents with sealants will improve overall effectiveness on all teeth,particularly on those teeth now thought of as difficult to seal. • Use of sealants has proved to have good results. • For prevention of dental caries in pit and fissure, sealants were introduced. • There is evidence suggesting effectiveness of sealants. • Sealants prevent bacteria growth which causes caries. • Biomaterials to seal pit and fissure should present with the simple application method, biocompatibility, low viscosity and good surface retention and low solubility. • To improve this biomaterial, more laboratory should be developed.
REFERENCES:
Essentials of Public Health Dentistry, Soben Peter (6th Edition).
FENESTRA 2002-18, Dr. Bruno Jacquot(Bruno.Jacqout@odonto.u-nancy.fr)
• Adenomatoid odontogenic tumor (AOT), generally considered to be an uncommon tumor • Occurs mostly in association with an unerupted maxillary cuspid. • Some investigators consider it as a benign neoplasm, while others have categorized it as a hamartomatous malformation due to the limited size and to the lack of recurrence of most cases (attributed perhaps to its minimal growth potential). • The AOT represents 3% to 7% of all odontogenic tumors.
• Although this lesion was formerly considered to be a variant of the ameloblastoma and was designated as “adenoma glioblastoma,” its clinical features and biologic behavior indicate that it is a separate entity.
PATHOPHYSIOLOGY: • There is evidence that the tumor cells are derived from enamel organ epithelium. • Investigators have also suggested that the lesion arises from remnants of dental lamina. • The specific stimulus that triggers proliferation of the progenitor cells of AOT is unknown. • Various hypotheses for the pathogenesis of AOT have been proposed. It could theoretically arise from the:
Enamel organ
The Epithelial lining of dentigerous cyst.
Epithelial rests of Malassez of the deciduous or permanent tooth
Remnants of the dental lamina.
CLINICAL FEATURES: • The mean age of these patients was approximately 18 years, with a range of 5-53 years. • However, 73% of the patient were under 20 years of age. • Marked predilection: in females 64%: males 36%. • Occurrence: greater in the maxilla (65%) than in the mandible (35%). • In contrast to the ameloblastoma, this tumor occurs more frequently in the anterior part of the jaws with 76% developing anterior to the cuspid in the maxilla and mandible. • Only very rarely does the lesion occur distal to the premolar area. • It is of some interest that in at least 74% of the cases, the tumors were associated with an unerupted tooth, and in over two-thirds of the cases, this tooth was the maxillary or mandibular cuspid. • Most tumors are relatively small, seldom exceed 3 cm in greatest diameter. • Although a few large lesions have been reported. • Peripheral (extraosseous) forms of the tumor are also encountered but are rare. • These usually appear as small, sessile masses on the facial gingiva of the maxilla. • Clinically, these lesions cannot be differentiated from the common gingival fibrous lesions.
***It is known astwo-third tumour: As it is seen : • 2/3rd in females. • 2/3rd in Anterior teeth region. • 2/3rd in impacted tooth region. • 2/3rd in cuspid region.
RADIOGRAPHIC FEATURES: • They are frequently asymptomatic , are discovered during the course of a routine radiographic examination or when films are made to determine why a tooth has not erupted. • Larger lesions cause a painless expansion of the bones. • In about 75% of cases, the tumor appears as a circumscribed, unilocular radiolucency that involves the crown of an unerupted tooth, most often a canine. • Follicular type of AOT may be impossible to differentiate radiographically from the dentigerous cyst. •Radiolucencyassociated with the follicular type of AOT sometimes extends apically along the root past the cementoenamel junction. • This feature may help to distinguish an AOT from a dentigerous cyst. • Less often the AOT is a well-delineated unilocular radiolucency that is not related to an unerupted tooth, but rather is located between the roots of erupted teeth (extrafollicular type) • The lesion may appear completely radiolucent: often, however, it contains fine (snowflake) calcifications. • Rare, multilocular cases have been reported and a scalloped border is observed occasionally. • Most cases are between 1 and 3 cm in greatest diameter. About 65% of reported cases also demonstrate faintly detectable radiopaque foci within the radiolucent lesion. • Occasionally, a more obvious intralesional radiopacity may be identified, usually eccentrically positioned within the lesion. • Divergence of roots and displacement of teeth occurs more frequently than root resorption. • Orbital and maxillary sinus encroachment have been reported. • Gingival lesions may cause slight erosion of the underlying alveolar bone cortex.
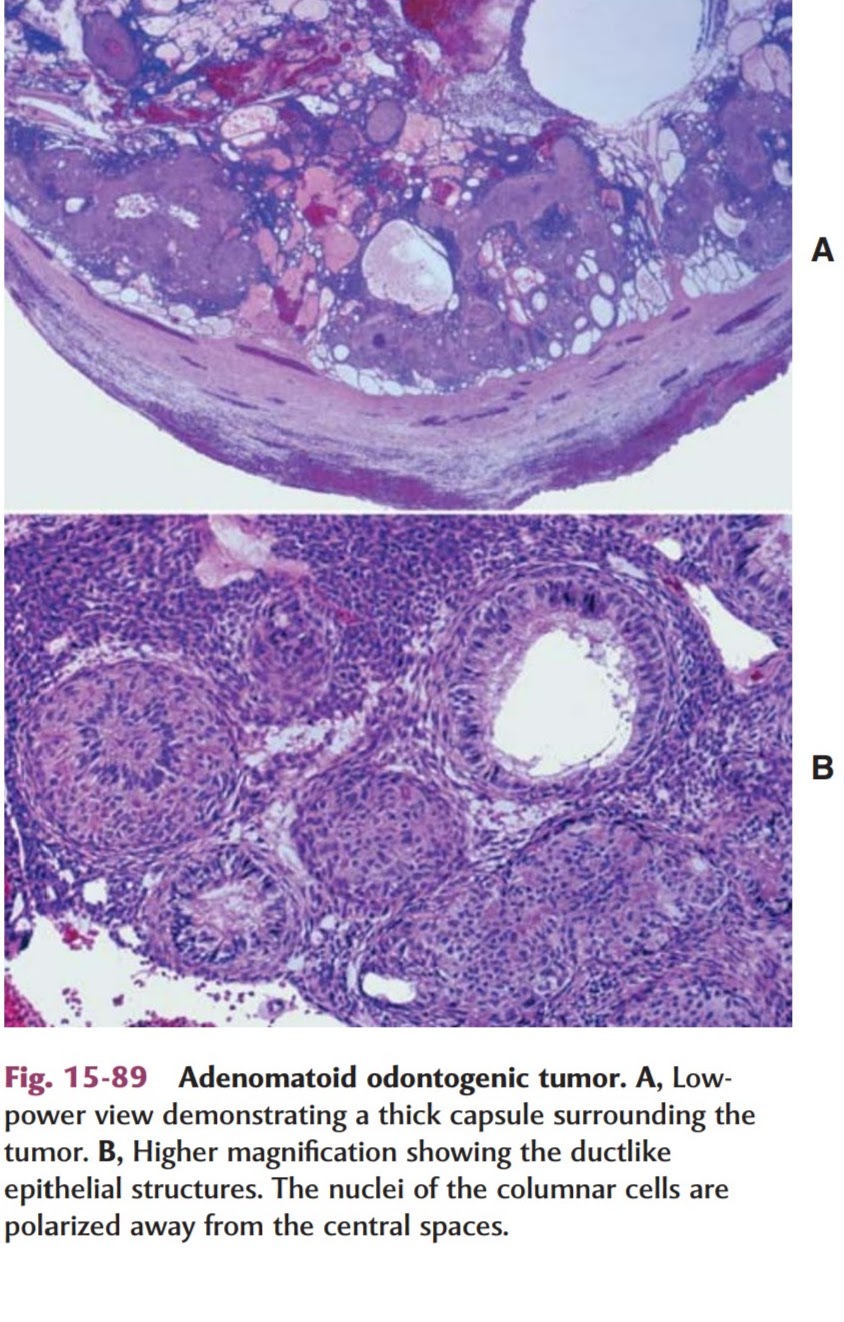
HISTOLOGICAL FEATURES: • AOT is a well-defined lesion that is usually surrounded by thick capsule. • When the lesion is bisected the central portion of the tumor may be essentially solid or may show varying degrees of cystic change. • Microscopically , the tumour composes of spindle shaped epithelial cells that form sheets, strand, or whorled masses of cells in a scant fibrous stroma • The epithelial cells may form rosette like structures about a central space, which may be empty or contain small amounts of eosinophilic material. • This material may stain for amyloid. • The tubular or duct like structures, which are the characteristic feature of the AOT, may be prominent, scanty, or even absent in a given lesion. • Lesion may consist of a central space surrounded by a layer of columnar or cuboidal epithelial cells. • The nuclei of these cells tend to be polarized away from the central space. • Small foci of calcification may also be scattered throughout the tumor. • These have been interpreted as abortive enamel formation. • Some tumours may contain larger areas of matrix material or calcification. • This material has been interpreted as dentinoid or cementum. • Some lesions also have another pattern, particularly at the periphery of the tumor adjacent to the capsule. • This consists of narrow, often anastomosing cords of epithelium in an eosinophilic, loosely arranged matrix.
TREATMENT & PROGNOSIS: • AOT is completely benign: because of its capsule, it enucleated easily from the bonc • Aggressive behavior has not been documented. • Recurrence after enucleation seldom, if ever, occurs.
REFERENCES: • Shafer’s Textbook of Oral Pathology (6th Edition). • Textbook of Oral Pathology, Neville (3rd Edition). • Manual of Oral Histology & Oral Pathology, Maji Jose.
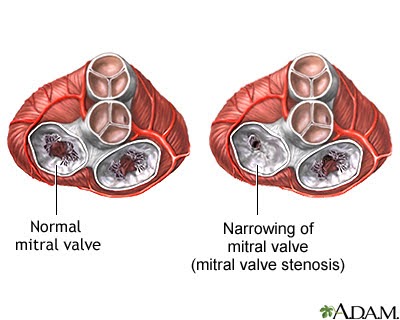
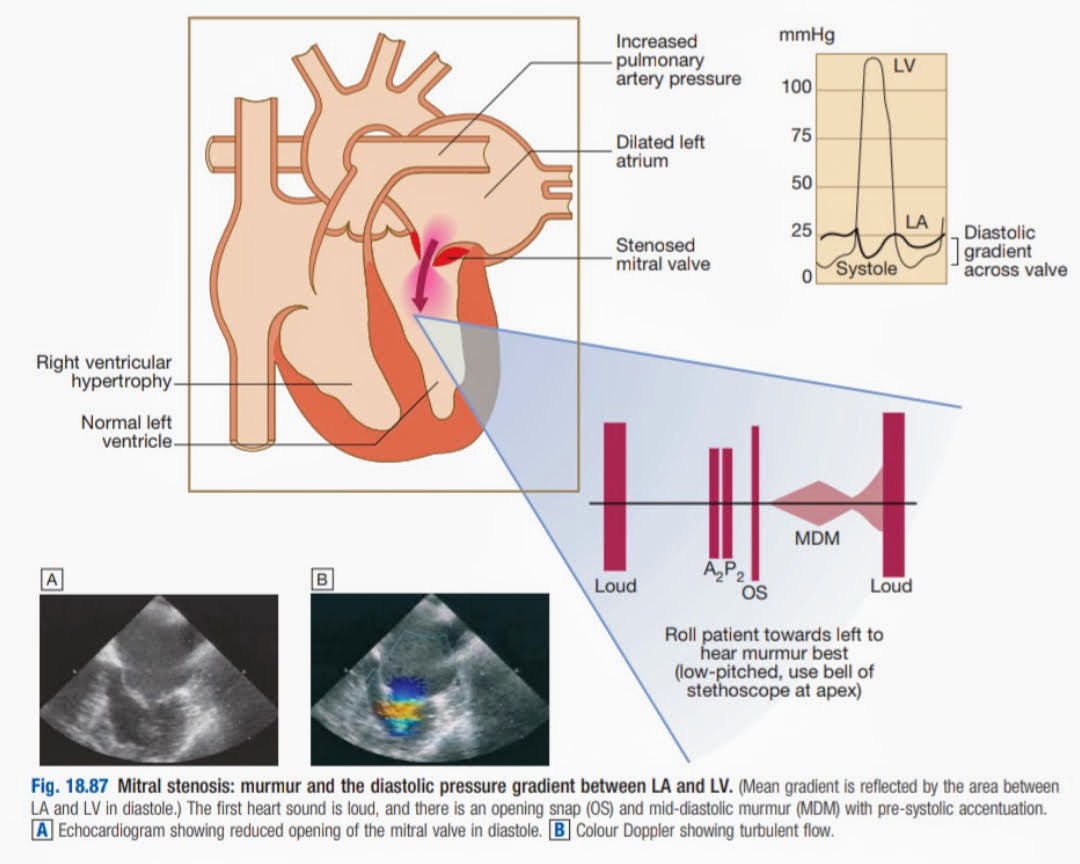
• The mitral valve apparatus is a funnel-shaped structure with its apex beat on the left ventricle. • Mitral Stenosis is the narrowing of the mitral valve of the heart. • Leads to complications due to the impairment of blood flow • More commonly seen in females. • Most Common cause : Rheumatic Heart Disease.
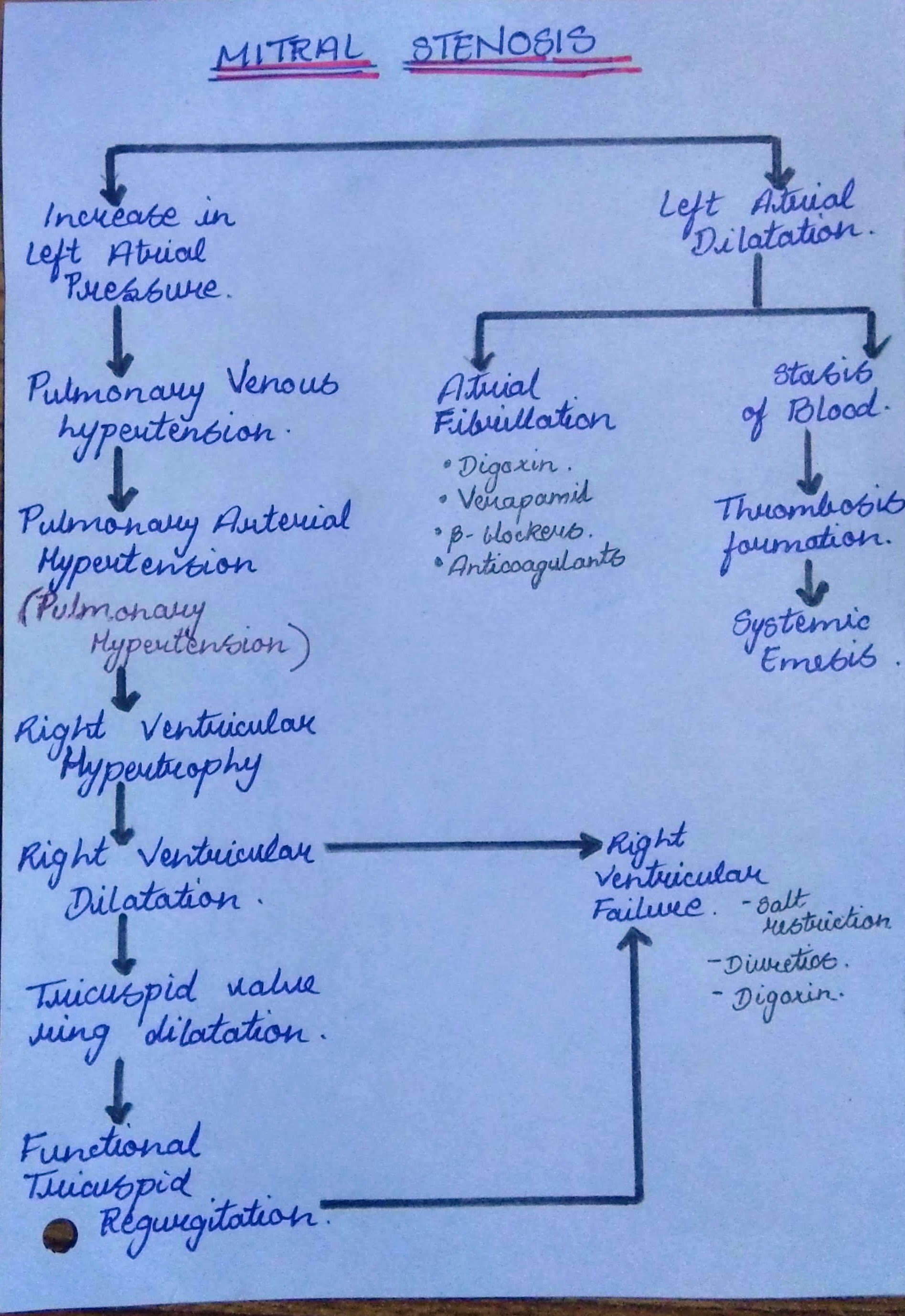
PATHOPHYSIOLOGY OF MITRAL STENOSIS ***Management of Atrial Fibrillation & RVF is written in bullet points for easier understanding
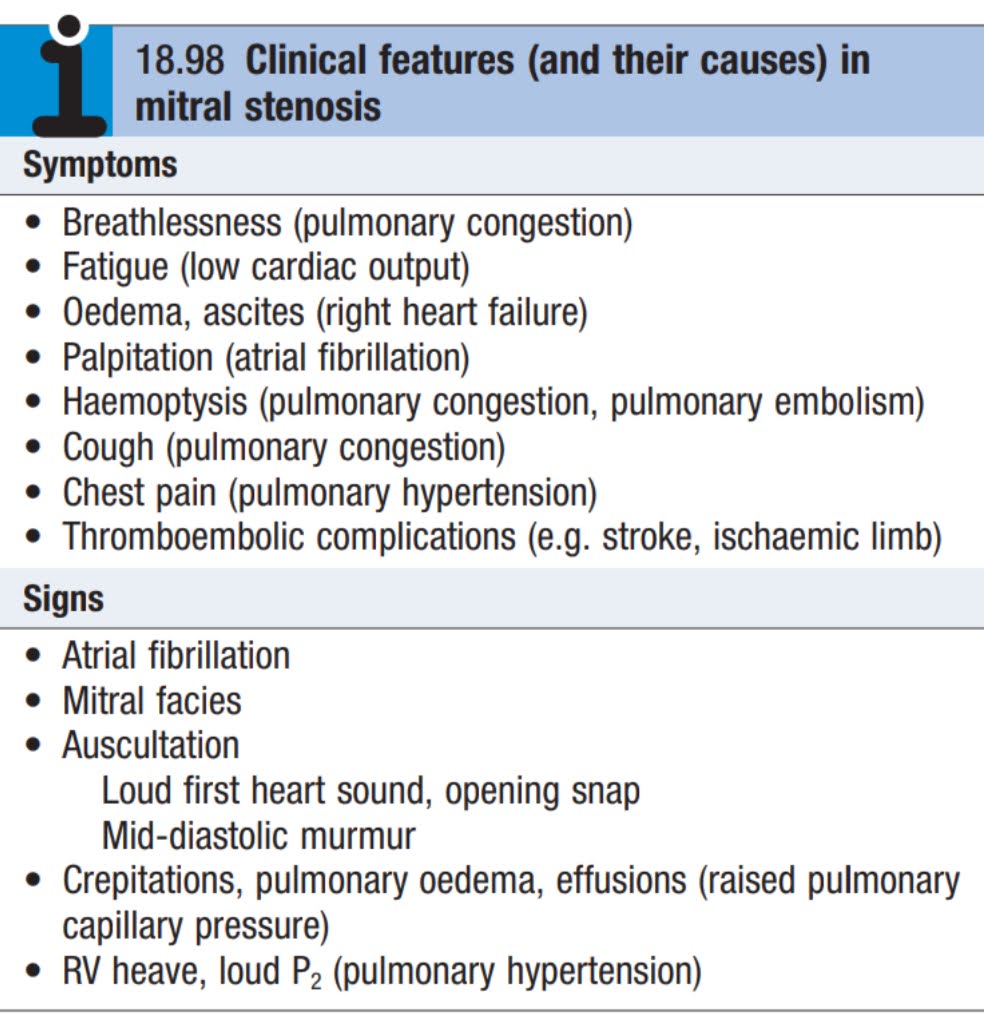
CLINICAL FEATURES: • Early presentation of Mitral stenosis include breathlessness on exertion and fatigue. • As stenosis progresses, patients are dyspnic on rest. • They have orthopnoea & paroxysmal nocturnal dyspnoea. • Acute pulmonary oedema may occur. • Haemoptysis: due to rupture of pulmonary-bronchial connection. • Edema of lower limbs. • Thromoembolic events like stroke, limb ischaemia • Winter bronchitis: Patient with myocardial infarction are prone to recurrent attacks of bronchitis, particularly during winters.
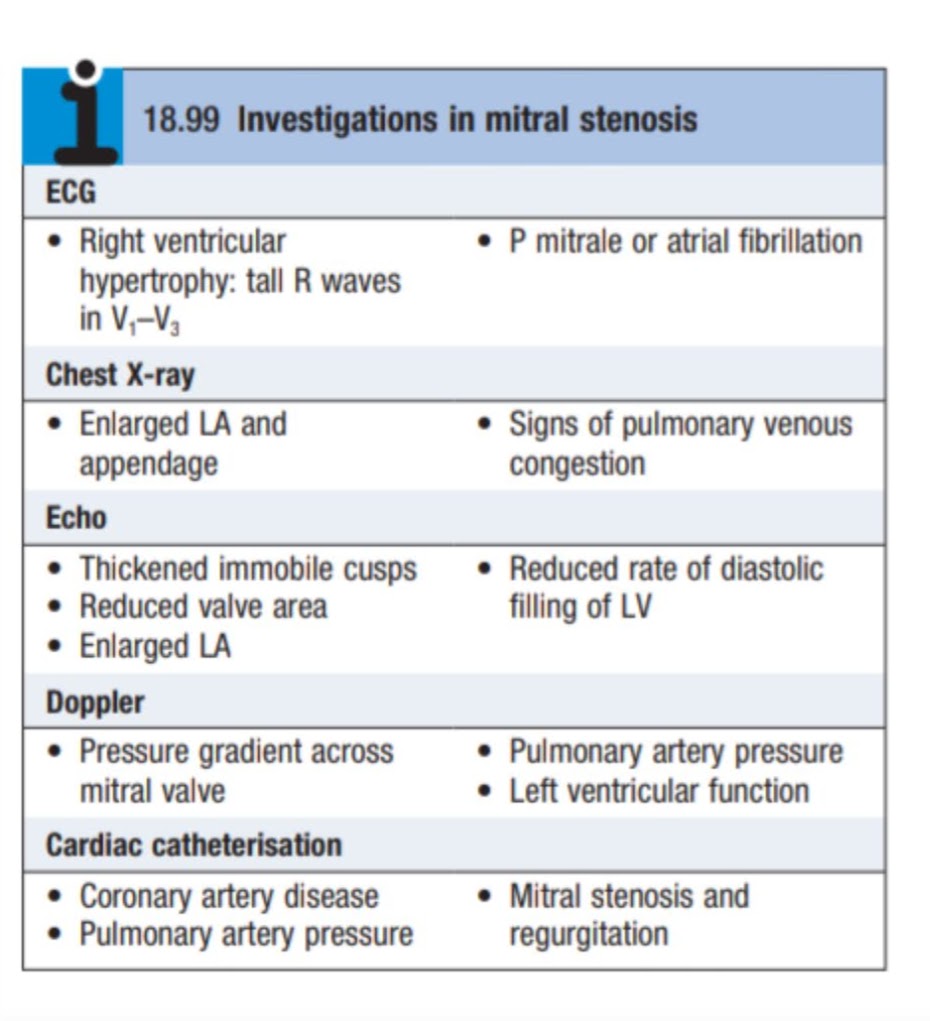
INVESTIGATIONS:
• ECG: May indicate left atrial(LA) enlargement, right ventricular hypertrophy and atrial fibrillation. • CHEST X-RAY: LA enlargement, pulmonary congestion. • ECHOCARDIOGRAPHY: Most sensitive & specific non-invasive methods to diagnose valvular disease.
May reveal structural abnormalities of the valve.
Size of cardiac chambers.
Pulmonary artery pressure.
Ventricular dysfunction & presence of thrombi.
CARDIAC CATHETERIZATION: Used to assess associated valvular lesions & to detect coronary artery disease.
4. Prophylaxis should be given to all patients to prevent rheumatic fever.
5. Prophylaxis for Infective Endocarditis should be given prior to the procedure.
SURGICAL MANAGEMENT:
MITRAL VALVECTOMY
Percutaneous Balloon Valvotomy:
Indicated when mitral valve is non-calcified &without regurgitation.
Procedure involves passing of a catheter across the valve & inflation of the balloon to dilate the orifice.
Open Valvotomy:
Carried out in patients where balloon valvotomy is not possible or in cases with restenosis(*means that a section of blocked artery that was opened up with angioplasty or a stent has become narrowed again)
In this procedure, the fusion of the valve is loosened, Ca(calcium) deposits and thrombi are removed.
2. MITRAL VALVE REPLACEMENT: o Mitral Valve is replaced when there is critical mitral stenosis(<1cm² of orifice size) o And/or there is an associated significant mitral regurgitation. o Replacement done,when mitral valve is severely distorted & calcified.
COMPLICATIONS: o Atrial fibrillation o Pulmonary Hypertension o Right Ventricular Failure o Systemic thromboembolism o Winter Bronchitis o Ortner’s Syndrome
REFERENCES:
Davidson’s Principle and Practise of Medicine
Medicine Prep Manual for Undergraduate, K George Mathew(4th Edition)
• ART :Is defined as a minimally invasive care approach in preventing dental caries and stopping its further progression. (Jo E. Frencken, 2012) • It consists of two components: sealing caries prone pits and fissures and restoring cavitated dentine lesions with sealant restorations. • American Academy of paediatric Dentistry (AAPD) defines ART as “a dental caries treatment procedure involving the removal of soft, demineralized tooth tissue using hand instrument alone, followed by restoration of the tooth with an adhesive restorative material, routinely glass ionomer”. • ART may be used to restore and prevent caries in young patients, uncooperative patients, or patients with special health care needs or when traditional cavity preparation and/or placement of traditional dental restorations are not feasible. • ART is based on modern knowledge about minimal intervention, minimal invasion and minimal cavity preparation for carious lesions. • It is a procedure based removing carious tooth tissues using hand instruments alone and restoring the cavity with an adhesive restorative material.
PRINCIPLES: The two main principles of ART are:
Removing carious tooth tissues using hand instruments only
Restoring the cavity with a restorative material that sticks to the tooth. The reasons for using hand instruments rather than electric rotating handpiecesare:
• The use of a biological approach, which requires minimal cavity preparation that conserves sound tooth tissues and causes less trauma to the teeth. • The low cost of hand instruments compared to electrically driven dental equipment, • The limited of pain that reduces the need for local anesthesia to a minimum and reduces psychological trauma to patients, • Simplified infection control. Hand instruments can easily be cleaned and sterilized after every patient.
Currently ART is performed using glass ionomer as the restorative material. The reasons for using glass ionomer are: • The Glass-ionomer sticks chemically to both enamel and dentine, the need to cut sound tooth tissue to prepare the cavity is reduced, • Fluoride is released from the restoration which will prevent and arrest caries and • It is rather similar to hard oral tissues and does not inflame the pulp or and does not inflame the pulp or gingiva
INDICATIONS: ART is carried out : • Only in small cavities (involving dentin). • In those cavities that are accessible to hand instruments. • Public Health programs • In cases when routine dental treatment cannot be performed because of a lack of facilities or accessibility to a dental clinic. • Can be used in schools as a community measure to control caries in a large number of children. • Can be used in both primary and permanent teeth.
CONTRAINDICATIONS: • There is presence of swelling (abscess) or fistula (opening from abscess to the oral cavity) near the carious tooth. • The pulp of the tooth is exposed. • Teeth have been painful for a long time and there may be chronic • Inflammation of the pulp, • There is an obvious carious cavity,but the opening is inaccessible to hand instruments • There are clear signs of a cavity, for example in a proximal surface, but the cavity cannot be entered from the proximal or the occlusal direction.
ADVANTAGES: • ART is a biological approach that requires minimal cavity preparation • It conserves sound tooth tissues and causes less trauma to teeth • As ART is painless the need for local anesthetics are reduced and so is the psychological trauma to patients. • Simplifies infection control as hand instruments can easily be cleaned and sterilized. • No electrically driven and expensive dental equipment needed which enables ART to be practiced in remote areas and in the field. • This technique is simple enough to train to train non- dental personnel or primary health care workers. • It is very cost effective. • As it is a friendly procedure, there great potentials for its use among children, fearful adults, physically and mentally handicapped and the elderly. • Makes restorable care more accessible for all the population groups.
ESSENTIAL INSTRUMENTS FOR ATRAUMATIC RESTORATIVE TREATMENT
MATERIALS: • ART is a treatment strategy that requires trained personnel and suitable materials for its success • ART is best performed using glass ionomer cement (GIC). • GIC (such as Fuji IX,GC Int) is a glass polyalkenoate cement that consists of calcium or strontium alumino-fluoro-silicate glass powder and water-soluble polymer. • Several factors led to the selection of GIC as a suitable material for ART. • These factors included its fluoride-releasing properties, its ability to bond to enamel and dentine, its pulpal biocompatibility, and its ease of manipulation. • The fluoride-release from GIC seems to be advantageous for ART Fluoride that is released from GIC makes the tooth structures (enamel and dentine) more resistant to acidic invasion by bacteria. • Fluoride can be released from glass ionomers for up to five years. • In addition, GIC acts as a reservoir for fluoride, as it takes up fluoride ions from topical fluoride This property of GIC means that the teeth treated with ART remain les susceptible to caries for long periods. A glass ionomer that in specifically designed for ART is available, which is termed a high-viscocity glass ionomer (such as Ketac Molar Easymix, 3M ESPE, Seefeld, Germany). It possesses a high powder-to-liquid ratio, with improved mechanical properties, including wear resistance, compressive strength, and marginal adaptability. A high-viscosity glass ionomer is the recommended type of glass ionomer for ART. A high viscosity glass ionomer is more durable than a low or medium-viscosity glass ionomer. Furthermore, a study performed in 2006 suggested that medium-viscosity glass ionomers should not be used in ART.
STEPS IN ART
SUCCESS RATE :
In 2001, a study was conducted in China regarding the success rate of ART performed on the primary teeth in various cavity designs 146). They found that, in 30 months of follow-up, the success rates were high for Class I and Class V restorations (79% and 70%, respectively). For Class II restorations, the success rate was found to be moderate. However, the success rates for both Class II and Class IV were found to be low .
Another study was performed in 2003 that showed that, in 24 months of follow-up, the success rate of ART performed in Class I cavities was high (89.6%). They also concluded that there was no significant difference in the success rate between ART and amalgam performed in Class I Cavities.
A meta-analysis was conducted in 2006 which addressed the success rates of ART in primary and permanent dentition. It concluded that, in 12 months of follow-up, the success rates of ART. made in the surfaces of single tooth and performed using high viscosity glass ionomer, were 95% and 97% for primary and permanent teeth, respectively.
Recently, a study was conducted in India addressing the success rate of ATR applied to one or two surfaces. They found that the success rate of ART was comparable to that of composite resins in 12 months of follow-up (89.7% for one surface and 88% for two surface restorations).
Regarding the method of the application of GIC in ART, a study was carried out in Brazil in 2016 which addressed the success rate of ART performed using a bilayer method 51. It concluded that the bilayer technique of ART increased the survival rate of proximal restorations in primary molars.
CONCLUSIONS: • Based on the available literature, we conclude that ATR is a suitable treatment approach for the management of dental caries in several conditions in both primary and permanent teeth. • ATR is used in cases where there are obstacles to reaching the dental care units • A high-viscosity glass ionomer performed better than low and medium-viscosity glass ionomers in ART. • Combining GIC with conditioner, as well as the use of the chemo-mechanical approach, improved the success rate of ART. • ATR is an acceptable strategy, with success rates comparable to the traditional treatment methods. REFERENCES: • Essentials of Public Health Dentistry, Soben Peter(6th Edition). • Atraumatic Restorative Treatment and Interim Therapeutic Restoration: A Review of the Literature(Dentist Journal). • Textbook of Preventive and Community Dentistry, Joseph John (3rd Edition).
Caused by Streptococcus pyogenes. B-hemolytic streptococci.
The disease begins as a streptococcal tonsillitis with pharyngitis in which the organisms elaborate an erythrogenic toxin that attacks the blood vessels and produces the characteristic skin rash.
The microorganism is present in the saliva/mucous spread by sneezing /coughing or direct contact with an infected person.
PATHOGENESIS
The rash is occurs by 3 endotoxins A,B & C:previously described as erythrogenic/scarlet fever toxins.
•It is suggested that development of scarlet fever may reflect a Hypersensitivity reaction required to exposure of skin.
CLINICAL FEATURES: • Scarlet fever is most common in children from the ages of 3 to 12 years. • The entry of microorganism occurs through the pharynx. • Incubation period :3-5days. • After this, the patient shows symptoms like severe pharyngitis & tonsillitis, chills, headache, abdominal pains and vomitting. • Also enlargement & tenderness of cervical lymph nodes is seen. • The diagnosis is not established until the characteristic – scarlet skin rash appears on the skin 2-3 days of illness. • This rash is prominent in the areas of skin folds, is a result of toxic injury to the epithelium. • Produces dilatation of small vessels and consequent hyperaemia. • Small papules of normal colour erupt giving a characteristic sandpaper texture to the skin. • Rash particularly in areas of skin fold is k/a Pastia lines. • Rash subsides after 6-7 days, followed by the desquamation of palms and soles. • Colour: Scarlet – Dusky Red
PASTIA LINES
ORAL MANIFESTATIONS: • Chief oral manifestation is referred to as stomatitis scarlatina. • Small punctuate red macules seen on hard palate, soft palate & uvula, k/a Forcheimmer Spots. • These are not diagnostic, as they may be present in other conditions like Rubella, Roseola & Infectious Mononucleosis • Palate and throat are often fiery red. • In early course of the disease, tongue exhibits white coating & the fungiform papillae are oedematous. • This phenomenon is k/a Strawberry tongue. • Coating is lost -the tip & lateral margins of tongue become deep red, glistening & smooth k/a Raspberry Tongue. • In severe cases, ulceration occurs on the buccal mucosa & palate, has been reported due to secondary infection.
DIAGNOSIS: • A culture of throat secretions may be used to confirm the diagnosis of streptococcal infection. • But this has been replaced by several methods of rapid detection of antigens that are specific for group A, B-hemolytic streptococci. • Failure to respond to appropriate antibiotics should alert the clinician that the detected strep tococci may represent an intercurrent carrier state. • Other causes of infection should be investigated. TREATMENT & PROGNOSIS: • Treatment of scarlet fever and the associated streptococcal pharyngitis is necessary to prevent the possibility of complications, such as peritonsillar or retropharyngeal abscess, sinusitis, or pneumonia. • Late complications are rare: Include otitis media, acute rheumatic fever, glomerulonephritis, arthralgia, meningitis, and hepatitis. • The treatment of choice is oral penicillin. • Erythromycin reserved for patients who are allergic to penicillin. • Ibuprofen can be used to reduce the fever and relieve the associated discomfort. • The fever and symptoms show dramatic improvement within 48 hours after the initiation of treatment. • With appropriate therapy, the prognosis is excellent.