What Do Radiographs Really Decide in Treatment Planning?
“If you see an impacted canine on an OPG, what makes you say— expose it… or extract it?”
This is a question every orthodontic student struggles with.
We are taught to look at angulation, height, overlap, resorption, and yet—when real consultants make decisions, only two radiographic factors consistently matter.
This blog breaks down which radiographic features truly influence treatment decisions and why, based on the classic study by Stivaros & Mandall (2000).
🔍 Why This Topic Matters Clinically
Impacted maxillary canines occur in 1.7–2.2% of the population.
Once a patient presents late, the orthodontist must choose between:
- Surgical exposure + orthodontic alignment
- Surgical removal
The wrong decision can mean:
- Prolonged treatment
- Periodontal compromise
- Failed alignment
- Unnecessary extraction
📌 Radiographs guide this decision—but not in the way students often assume.
🧠 Study in One Line
Orthodontists do NOT base their decision on most OPG measurements.
Instead, they rely mainly on:
- Labio-palatal position of the canine crown
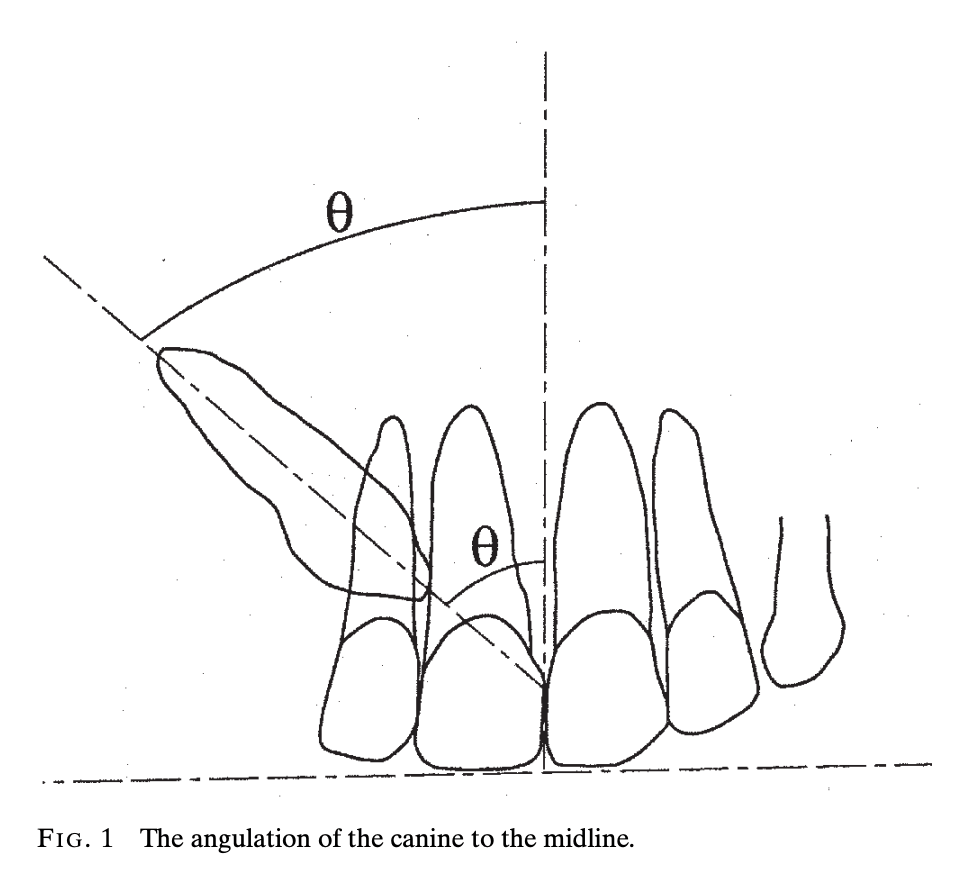
- Angulation of the canine to the midline
🖼️ Radiographs Used in Decision Making
| Radiograph | Purpose |
|---|---|
| OPG | Angulation, vertical height, overlap, root position, resorption |
| Lateral Skull Radiograph | Labio-palatal position of crown & root |
📐 Radiographic Variables Assessed
1️⃣ Canine Angulation to Midline (OPG)
| Grade | Angulation |
|---|---|
| Grade 1 | 0–15° |
| Grade 2 | 16–30° |
| Grade 3 | ≥31° |
📌 Key Insight:
As angulation increases → probability of extraction increases
2️⃣ Vertical Height of Canine Crown
| Grade | Position Relative to Incisor |
|---|---|
| 1 | Below CEJ |
| 2 | Above CEJ but < ½ root |
| 3 | > ½ root but < full root |
| 4 | Above full root length |
⚠️ Surprising finding:
Vertical height did NOT significantly influence the treatment decision.

3️⃣ Overlap of Adjacent Incisor Root
| Overlap | % Cases |
|---|---|
| No overlap | 13.6% |
| Complete overlap | 55.6% |
| Grade | Description |
|---|---|
| Grade 1 | No horizontal overlap of the incisor root |
| Grade 2 | Overlap of less than half the width of the incisor root |
| Grade 3 | Overlap of more than half, but less than the full width of the incisor root |
| Grade 4 | Complete overlap of the incisor root width or more |
🧠 Clinical myth busted:
Even severe overlap did not statistically affect whether the canine was exposed or removed.

4️⃣ Root Resorption of Adjacent Incisor
| Status | % Cases |
|---|---|
| Present | 22.7% |
| Absent | 77.3% |
📌 Detected only on OPG → bucco-lingual resorption often missed.
⭐ The MOST Important Factor:
Labio-Palatal Position of the Canine Crown
| Crown Position | Exposed (%) | Removed (%) |
|---|---|---|
| Labial | 0 | 100 |
| Line of arch | 20 | 80 |
| Palatal | 66.7 | 33.3 |
🔑 Why Palatal Canines Are Favored for Exposure
- Better gingival management
- Easier surgical access
- Closed eruption techniques easier to manage
- Less risk of attachment failure
👉 Labial canines = poor periodontal prognosis → extraction preferred
📊 What Logistic Regression Showed
| Radiographic Factor | Influence on Decision |
|---|---|
| Labio-palatal crown position | ✅ Significant |
| Canine angulation to midline | ✅ Significant |
| Vertical height | ❌ Not significant |
| Incisor overlap | ❌ Not significant |
| Root resorption | ❌ Not significant |
🧠 Clinical Interpretation (Exam-Gold Section)
Despite multiple measurable radiographic parameters, orthodontists subconsciously prioritize what affects biomechanics and periodontal outcomes the most.
- A palatally placed canine can often be guided into the arch safely.
- A horizontally angulated canine fights biomechanics.
- OPG measurements act as guides, not decision-makers.
📝 Questions to Ponder (with Answers)
❓1. Why doesn’t severe incisor overlap automatically lead to extraction?
Answer:
Modern fixed orthodontics allows alignment even from difficult positions. Overlap alone does not predict failure.
❓2. Why is labial impaction considered worse than palatal?
Answer:
Because of:
- Attached gingiva loss
- Higher risk of gingival recession
- Difficulty with surgical access and rebonding
❓3. Why is angulation more important than vertical height?
Answer:
Angulation determines path of eruption and biomechanical feasibility, whereas height mainly affects treatment duration.
❓4. Why can’t OPG alone decide treatment?
Answer:
OPGs have:
- Magnification
- Distortion
- Poor bucco-lingual information
👉 Lateral skull radiograph adds crucial spatial insight.
❓5. If radiographs are limited, what else influences decisions?
Answer:
- Patient motivation
- Oral hygiene
- Periodontal status
- Willingness for long treatment
🎯 Take-Home Message for Students
Don’t get lost measuring everything on an OPG.
Ask yourself just two questions first:
1️⃣ Is the canine palatal or labial?
2️⃣ How steep is its angulation to the midline?
Everything else is supporting data—not the final verdict.

