When we think of Class III malocclusion, our minds instantly jump to “mandibular prognathism,” “maxillary deficiency,” or that unmistakable concave profile. But what if we told you that the story begins much deeper—in a region most clinicians rarely visualize: the cranial base.
A fascinating study by Chang et al. (2005) reveals how subtle changes in the cranial base shape can quietly set the stage for a Class III facial pattern long before the first molar even erupts.
🔍 Why the Cranial Base Matters
The cranial base serves as the architectural foundation for:
- The position of the mandible
- The forward placement of the maxilla
- TMJ inclination
- Facial profile development
Think of it as the “orthodontic motherboard.”
If it develops differently, everything built upon it shifts.
1. The Big Finding: A Shorter Posterior Cranial Base
The study compared 100 Class III children with 100 normal controls. The most striking difference?
👉 The posterior cranial base was significantly shorter in Class III subjects.
This included reduced:
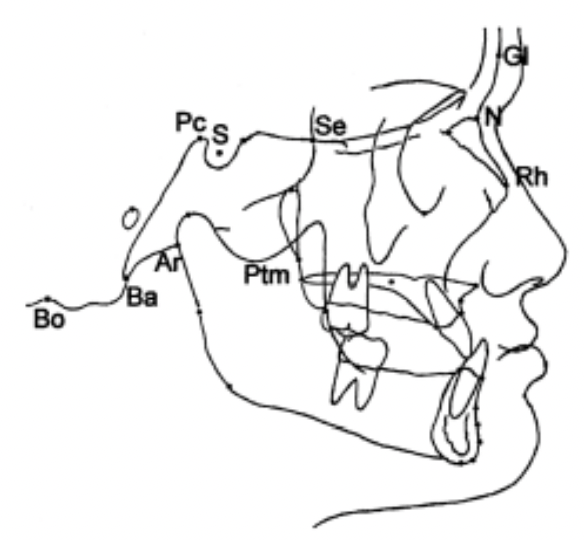
- S–Ar
- Pc–Ar
- Pc–Ba
- Pc–Bo
- Ar–PM
- Bo–PM
This matters because the posterior cranial base guides the position of the condyle.
A short base = the TMJ sits more forward → the mandible follows → Class III appearance emerges.
Clinically:
Ever seen a child with mild mandibular projection but no clear functional shift?
Think posterior cranial base deficiency.
2. The Saddle Angle Story: More Acute Angulation
The study found:
- N–S–Ar and N–Pc–Ar angles were more acute in Class III children.
This means the cranial base is more bent—a phenomenon sometimes called “cranial base kyphosis.”
Why it matters:
A more acute saddle angle shifts the glenoid fossa forward → the mandible comes along for the ride.
This is a skeletal pattern—not a habit, not a posture.
4. The Cranial Base Pattern Is Set Early—Very Early
Several classic studies say show that:
- Cranial base shape develops prenatally
- The saddle angle remains remarkably stable through childhood
- Variations appear early and persist
This explains why:
- Class III patterns often run in families
- Interceptive treatment is most effective before growth accelerates
- Prediction of Class III progression often depends on baseline cranial-base morphology
Final Thought
Class III malocclusion is not simply a “big mandible vs small maxilla” problem.
It’s a developmental story—one rooted in the very foundation of the skull.
Understanding cranial-base morphology gives orthodontists a sharper lens to diagnose, counsel, and treat Class III patients—particularly in their formative years.
Growth & Treatment Planning Hints
- Shortened, flexed posterior cranial base
→ Expect stronger skeletal Class III tendency.
→ Earlier interceptive approaches (facemask + RME, chincup, functional orthopedics) may be more justified. - Cranial base near normal, but Class III present
→ Consider dominant roles of maxillary retrusion, mandibular overgrowth, or local factors.
- Rapid visual check on lateral ceph
- Look at posterior base: S‑Ar, Pc‑Ar, Pc‑Ba, Ar‑PM, Ba‑PM, Bo‑PM.
- Assess saddle region: N‑S‑Ar and N‑Pc‑Ar.
- Scan midface profile: Gl‑N‑Rh.


