When a maxillary lateral incisor is missing, substituting the canine into its place can produce excellent esthetic and functional results — but only if torque control is done right. One of the most common errors? Inadequate palatal root torque in the relocated canine.
Why Torque Matters
The canine crown is bulkier, and without enough palatal root torque, its prominence can disrupt smile esthetics and compromise occlusion. The right bracket choice helps counteract this.

Bracket Options & Prescriptions (MBT*)
| Bracket Choice | Torque / Tip | Key Advantages | Notes |
|---|---|---|---|
| Maxillary Central Incisor | +17° torque / 4° tip | Maximum palatal root torque | Enameloplasty needed; add up to +4° distal root tip |
| Maxillary Lateral Incisor | +10° torque / 8° tip | Good torque & tip control; easy placement | Enameloplasty needed |
| Flipped Maxillary Canine | +7° torque / 8° tip | Torque & tip control without reshaping | May not give enough torque |
| Flipped Mandibular 2nd Premolar | +17° torque / 2° tip | Max torque without enameloplasty | Remove bracket posts after bonding |
*Modified for Roth or Damon prescriptions if needed.
Torque Tips
- “1 to 5 Rule”: Every .001″ slot–wire play ≈ 5° torque loss
- .017″×.025″ in .018″ slot → 5° loss
- .019″×.025″ in .022″ slot → 10–15° loss
- This is why an .018 slot system with .017×.025 wire tends to have better torque control than a .022 slot with .019×.025 wire, assuming same bracket prescription.
- If you want to minimize torque loss, you either:
- Use the largest possible wire for that slot
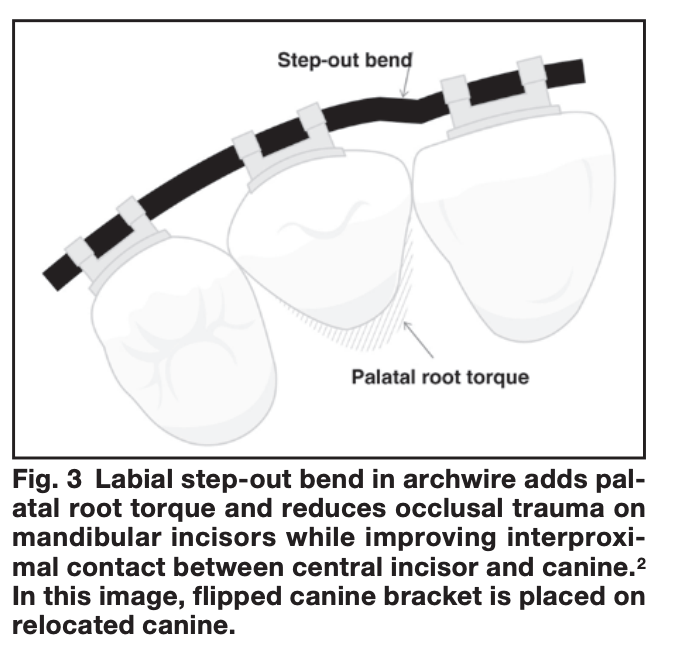
- Or add auxiliary torque (e.g., torquing springs, step-out bends)
- Labial step-out bend → adds palatal root torque + avoids traumatic contact.
- Labial step-out bends shift the canine root palatally, improving torque and interproximal contact while minimizing occlusal interference.
Example 1: .017″ × .025″ wire in a .018″ slot
- Slot height = 0.018″
- Wire height = 0.017″
- Difference (play) = 0.001″
- Torque loss = 0.001″ × 5° = ≈ 5° loss
So even with a nearly full-size wire, you can’t get 100% torque expression — there’s some rotational freedom before the wire contacts the slot walls.

Example 2: .019″ × .025″ wire in a .022″ slot
- Slot height = 0.022″
- Wire height = 0.019″
- Difference (play) = 0.003″
- Torque loss = 0.003″ × 5° = ≈ 15° loss
Why the guide says 10–15° instead of exactly 15°:
- Theoretical loss = 15° (from math)
- In practice, clinical torque loss is often slightly less because:
- Residual tip in the tooth means the wire contacts sooner than expected
- Manufacturing tolerances (slots often oversized, wires slightly undersized or rounded)
- The wire may seat differently under ligation forces
Other Factors Influencing Torque
- Archwire material (SS > TMA > NiTi for high torque)
- Bracket material
- Type of ligation
- Interbracket distance
- Tooth morphology & biology
Clinical Pearls
- Delay enameloplasty if unsure → choose flipped mandibular 2nd premolar for torque & base fit.
- Canine extrusion improves gingival architecture but monitor occlusion.
- For high torque (>24°), beta titanium is safer than SS for bends.
- Beta titanium offers a balance between torque delivery and flexibility, making it preferable for large bends compared to the stiffness of stainless steel.
📌 Reference: Kravitz ND, Miller S, Prakash A, Eapen JC. Canine Bracket Guide for Substitution Cases. J Clin Orthod. 2017;51(8):452-455.

