🚀 Imagine this:
You’re treating a teenage patient with:
- A deep curve of Spee,
- Mild arch length deficiency (~1–2 mm),
- And an anterior crowding with slightly flared lower incisors.
You’re not quite ready for extractions, and distalization isn’t needed in full force. You just need a smart trick to upright the molars and gain that precious 1–2 mm of space per side. What do you do?
Enter the Tip-Back Mechanism.
🎯 What Is the Tip-Back Mechanism?
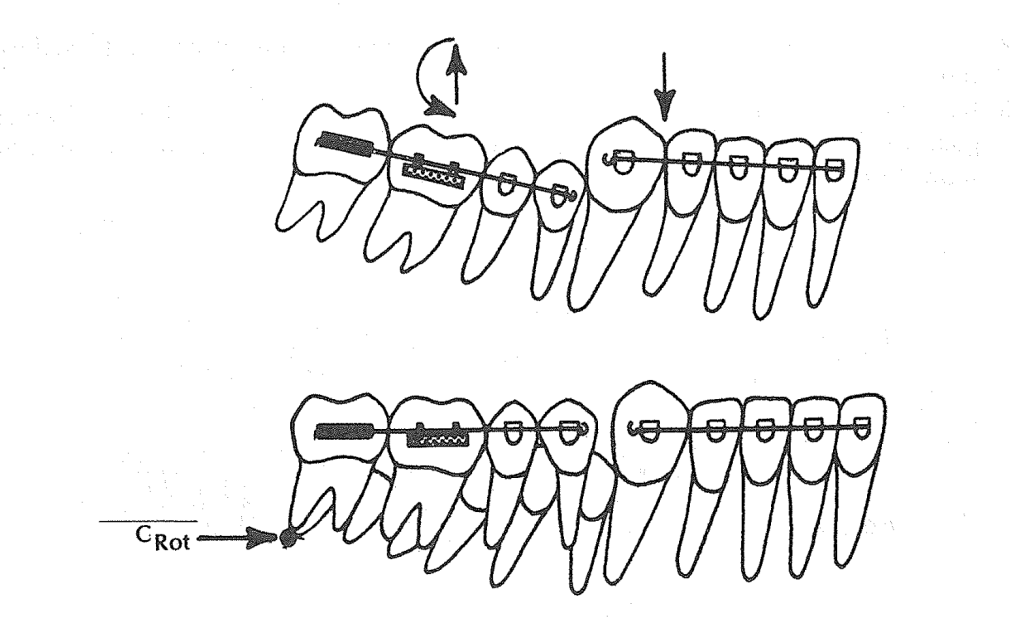
Think of the tip-back spring like a little lever system. It uses a negative moment to rotate the buccal segments (molars and premolars) upright, making them more vertical instead of tipped mesially.
When you do that, the buccal segments “tip back”, and voilà – a small but meaningful amount of arch length is gained anteriorly.
Key term: Crot (center of rotation) – in this case, found distal to the second molar, allowing effective rotation and eruption of the buccal segment.
🛠️ Components of a Tip-Back Setup
Here’s what goes into this appliance:
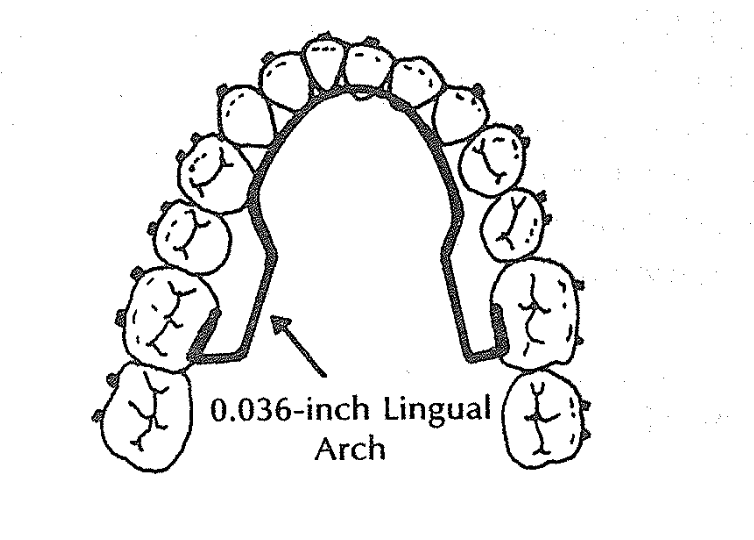
- 0.036” Lingual Arch – for anchorage.
- 0.018 × 0.025” Anterior Segment – typically from lateral to lateral or lateral to premolar.
- Buccal Stabilizing Segments (BSS) – rectangular wires (0.018 × 0.025”) from molars to premolars.
- The Tip-Back Hook/Spring – placed strategically to apply the eruptive & rotational force.
✅ Scenario 1: Hook Placed Between Canine and Lateral Incisor (Near CRes of Anterior Segment)
Patient: 13-year-old with mild lower incisor crowding, deep bite, and normal axial inclination of anteriors.
Clinical Findings:
- Deep curve of Spee
- Lower incisors are upright
- Mandibular canines and lateral incisors are aligned but crowded
- Slight arch length deficiency (~2 mm)
Hook Placement:
👉 Between lateral incisor and canine, i.e., near the center of resistance (CRes) of the anterior segment.
Biomechanical Reasoning:
- When the hook is placed close to the CRes, the force system causes minimal rotational tendency on the anterior segment.
- This results in controlled tip-back and uprighting of the molars without flaring or retraction of incisors.
- Eruptive force is delivered to molars → distal crown tipping → space is gained mesial to first premolars.

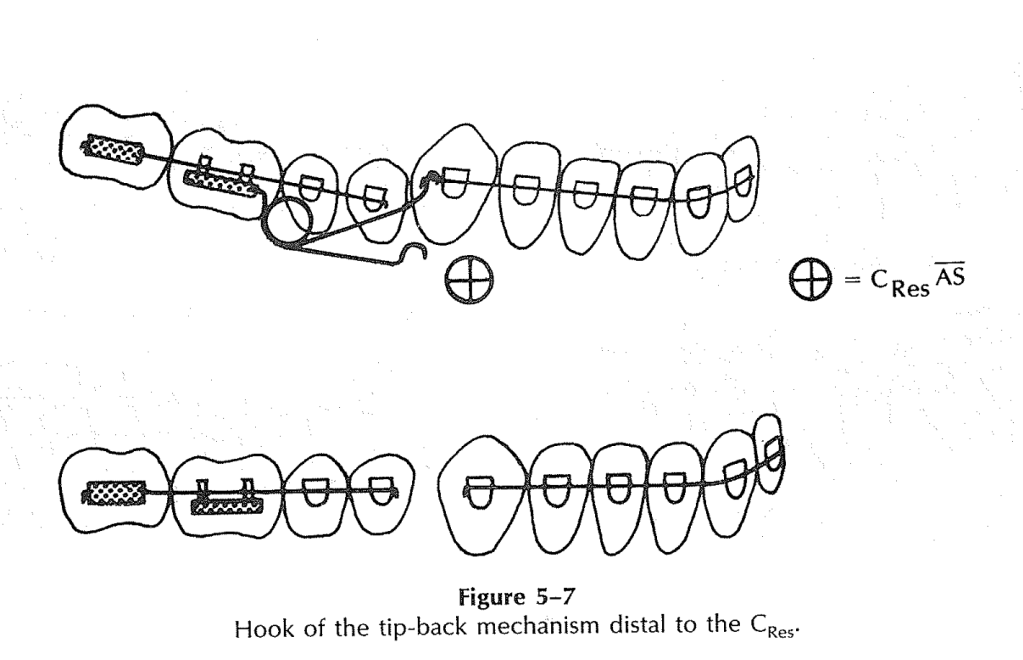
✅ Scenario 2: Hook Placed Distal to the Canine (Distal to the CRes of Anterior Segment)
Patient: 14-year-old with pseudo-Class III tendency and flared lower incisors
Clinical Findings:
- Lower incisors show labial flaring
- Canines are slightly higher (gingivally placed) than central incisors
- There is mild lower anterior crowding
- Patient shows forward functional shift of the mandible
Hook Placement:
👉 Distal to the CRes—typically between canine and first premolar
Biomechanical Reasoning:
- Force acts below and behind the CRes of the anterior segment.
- This creates a clockwise moment, causing the roots of the incisors to come forward, helping to upright flared anteriors.
- It counteracts the labial inclination, resulting in a flatter occlusal plane.
📚 Summary: When to Use Tip-Back?
Use this when your case has:
- 🧑⚕️ A growing patient,
- 😬 Deep curve of Spee,
- 📏 Mild arch length deficiency (1–2 mm),
- 🦷 Steep occlusal plane,
- 🚫 Need to avoid anterior flaring.
| Scenario | Hook Placement | Effect on Anterior Segment | Clinical Use |
|---|---|---|---|
| 1 | Between lateral incisor & canine | Neutral / minimal tipping | Deep bite, normal incisor inclination |
| 2 | Distal to canine | Uprighting of flared anteriors | Pseudo-Class III, flared lower incisors |

