Bimaxillary protrusion is a condition characterized by protrusive and proclined upper and lower incisors with increased lip procumbency. It is commonly seen in African-American and Asian populations but can occur across all ethnic groups. Due to the negative perception of protrusive dentition and lips in many cultures, patients with bimaxillary protrusion often seek orthodontic treatment to improve their facial profiles. This guide summarizes key aspects of bimaxillary protrusion, including its etiology, pretreatment characteristics, treatment goals, and outcomes.
Etiology of Bimaxillary Protrusion
The etiology of bimaxillary protrusion is multifactorial, including:
- Genetic Factors: Hereditary traits influencing facial and dental structures.
- Environmental Factors:
- Mouth breathing.
- Tongue and lip habits.
- Increased tongue volume.
Morphological Features
Keating’s study on Caucasian patients identified the following cephalometric traits:
| Feature | Observation |
|---|---|
| Posterior cranial base | Shorter |
| Maxilla | Longer and more prognathic |
| Skeletal pattern | Mild Class II |
| Upper and posterior face height | Smaller |
| Facial planes | Divergent |
| Soft tissue profile | Procumbent with a low lip line |
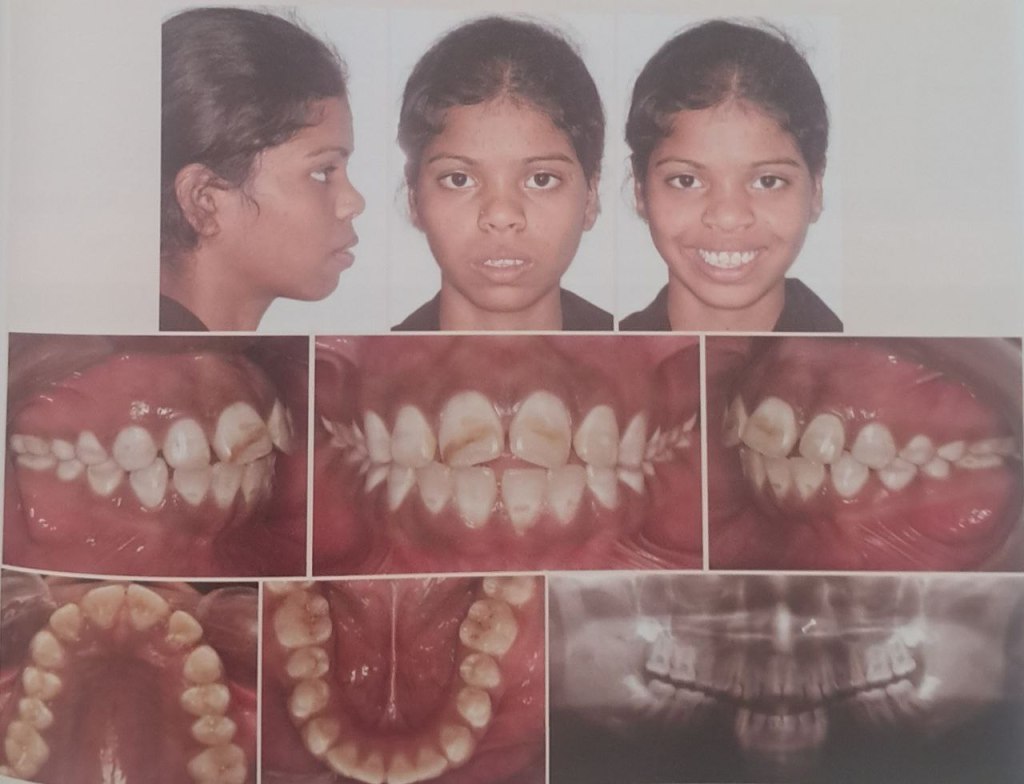
Pretreatment Characteristics
Cephalometric Traits
Patients with bimaxillary protrusion exhibit the following pretreatment characteristics:
| Trait | Observation |
| Upper and lower incisor proclination | Increased (2-3 SD above mixed racial norms) |
| Vertical growth patterns | Increased lower anterior face height |
| Mandibular plane angle | Elevated |
| Alveolar heights | Increased |
Soft Tissue Features
- Lip Position:
- Upper and lower lips are ahead of the E-plane.
- Lower lip: 6.0 mm ahead (Keating’s Caucasian sample).
- Upper lip: 1.0 mm ahead (less than Keating’s 3.4 mm).
- Nasolabial Angle:
- Found to be 94° (1 SD more acute than mixed racial norms).
- Tan’s study on Chinese patients reported an even more acute angle (86.6°).
- Lip Thickness:
- Increased, likely due to a higher proportion of African-American patients in the study.
Alveolar Morphology
- Alveolar Width: Reduced compared to Handelman’s norms.
- Alveolar Height: Increased, consistent with vertical facial growth patterns.
- Thin and elongated alveolus may limit retraction mechanics and necessitate surgical osteotomies in severe cases.
Orthodontic Treatment Goals
The primary objectives of treating bimaxillary protrusion include:
- Dental Goals:
- Retraction and retroclination of maxillary and mandibular incisors.
- Reduction in incisor proclination and protrusion.
- Soft Tissue Goals:
- Decrease in lip procumbency and convexity.
- Improvement in the nasolabial angle.
- Mechanics Used:
- Extraction of four first premolars.
- Retraction using maximum anchorage mechanics.
Flowchart: Treatment Goals and Process
1. Initial Diagnosis → 2. Extraction of Four Premolars → 3. Retraction of Incisors → 4. Profile Improvement
Treatment Outcomes
Dental and Skeletal Changes
| Parameter | Observation |
| Interincisal angle | Increased significantly |
| Incisor inclination | Decreased significantly |
| Anteroposterior incisor position | Reduced significantly (P < .001) |
Soft Tissue Changes
- Upper Lip Retraction:
- Ratio of upper incisor retraction to upper lip retraction: 2.2:1 (similar to Chiasson and Hershey).
- Nasolabial angle: Increased significantly (P < .02).
- Variability:
- Lip response depends on factors like interlabial gap, lip redundancy, and musculature quality.
Vertical Dimension
- No significant changes in lower anterior face height or mandibular plane angle, indicating that treatment mechanics do not affect the vertical dimension.

