Class III Malocclusion and Maxillary Retrusion
- Causes: Class III malocclusions can arise from mandibular protrusion, maxillary retrusion, or both.
- Studies on Maxillary Retrusion: Various studies report the contribution of maxillary retrusion to Class III malocclusions in individuals with normal mandibles, with percentages ranging between 19.5% and 37%.
- Treatment Focus: This recognition has led to introducing treatments like the orthopedic facemask for maxillary protraction.
Alternate Rapid Maxillary Expansion and Constriction (Alt-RAMEC)
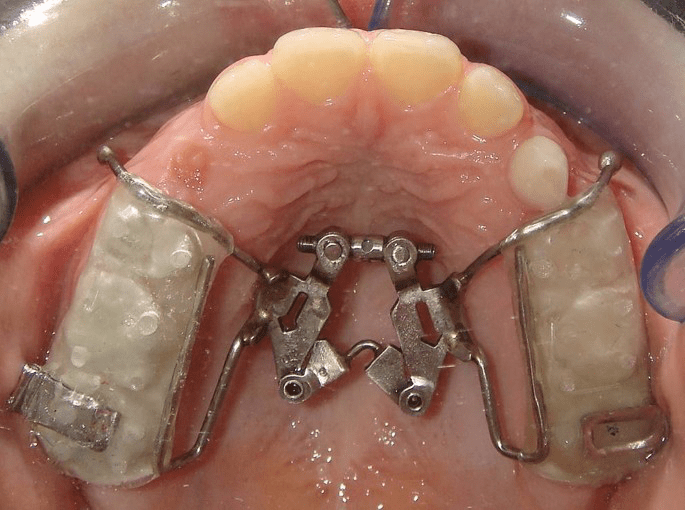
- Protocol: Expands and contracts the maxilla alternately (1 mm/day for a week each, repeated for 7–9 weeks) using a two-hinged rapid maxillary expander.
- Rationale: Mimics the rocking mechanism in tooth extraction, disarticulating circum-maxillary sutures without over-expansion.
Alt-RAMEC Protocol Details
- Activation Phase:
- The expansion screw was turned twice daily at a rate of 0.20 mm per turn.
- This phase lasted for 1 week, ensuring the maxilla was progressively expanded.
- Deactivation Phase:
- The screw was then turned twice daily in reverse at a rate of 0.20 mm per turn.
- This phase also lasted for 1 week, gradually constricting the maxilla back.
- Repetition:
- The activation and deactivation sequence was repeated for a second cycle.
- After each week-long activation or deactivation phase, the patients were examined to monitor proper opening or closing of the screw, ensuring precision in the procedure.
- Post-Protocol Guidance:
- Following the completion of the Alt-RAMEC cycles, patients were instructed to wear the Reverse Headgear (RH). This is a common adjunct in orthopedic facemask therapy designed to enhance maxillary protraction after the suture disarticulation achieved by Alt-RAMEC.
Results of Alt-RAMEC
- Comparison with RPE:
- Alt-RAMEC: Achieved an average anterior movement of point A by 5.8 mm in cleft patients over 9 weeks.
- RPE: Achieved only 2.6 mm movement after 1 week.
- Suture Opening: Experimental studies confirmed that Alt-RAMEC opens circum-maxillary sutures more extensively than 1 week of RPE.
Clinical Implications
| Parameter | A/D-RPE Group | RPE Group | Comparison with Previous Studies |
|---|---|---|---|
| Maxillary Advancement (Point A) | 4.13 mm (T3) | 2.33 mm (T3) | Greater movement in A/D-RPE group, similar to Liou and Tsai (2005) findings. |
| Anterior Movement of Point A | Significant difference (greater in A/D-RPE) | Observed, but lesser than A/D-RPE | Liou and Tsai (2005), Merwin et al. (1997), Kapust et al. (1998), Sung & Baik (1998) showed comparable results to RPE group. |
| Mandibular Rotation | Posterior rotation observed | Posterior rotation observed | Consistent with previous studies (Merwin et al., 1997; Kapust et al., 1998). |
| Anterior Face Height Increase | Observed | Observed | Findings align with previous studies. |
| Maxillary Plane Angle | Decrease of 1.53 degrees (T3) | Decrease observed | A/D-RPE showed significant decrease, consistent with previous studies. |
| SNA Angle Increase | Significant difference (greater in A/D-RPE) | Observed | A/D-RPE resulted in more significant SNA angle increase compared to RPE group. |
| ANB Angle Increase | Significant difference (greater in A/D-RPE) | Observed | A/D-RPE showed more significant increase in ANB angle. |
| Overjet Correction | Greater correction in A/D-RPE | 92.5% skeletal, 7.5% incisor tipping | A/D-RPE showed a higher skeletal contribution (93%) vs. RPE (92.5%). |
| Skeletal vs. Dental Contribution to Overjet | 93% skeletal, 7% dental | 92.5% skeletal, 7.5% dental | A/D-RPE showed a higher skeletal contribution (57.9% maxillary, 35.1% mandibular). |
| Soft Tissue Profile Changes | More pronounced in A/D-RPE (upper lip anterior, lower lip posterior) | Observed (less pronounced) | Profile improvement observed in both groups; A/D-RPE showed more pronounced soft tissue changes. |
| RH Usage During Treatment | 16-18 hours/day (initial 6 months), 12 hours/day (2nd 6 months), 6 hours/day (passive phase) | Varied by study, typically used for 14 hours/day | Similar to recommendations of Saadia and Torres (2000) and others (Macdonald et al., 1999). |
| Relapse | No significant relapse observed | No significant relapse observed | Consistent with previous studies (Macdonald et al., 1999; Vaughn et al., 2005). |

