

PALATAL ADVANCEMENT FLAP
- This technique is very similar to buccal advancement technique where the gingiva is close to the oroantral defect is mildly advanced to approximate it.
- May be done for small sized defects.
- It is not possible to get too much of advancement, as the palatal tissue is very rigid and thick.
- In this,the palatal tissue surrounding the OAC, is reflected +may be advanced downwards and sutured to the buccal tissue to cover the detect.
- Not a very successful procedure.
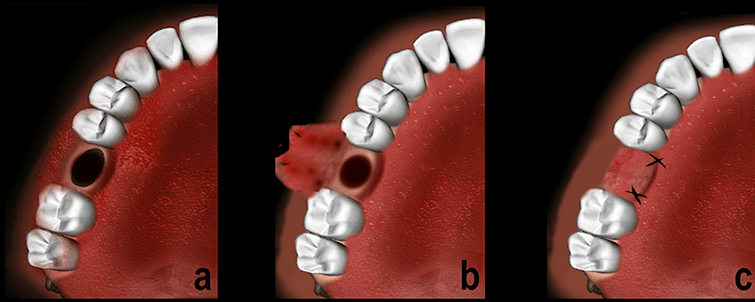
ROTATIONAL ADVANCEMENT FLAP or ASHLEY’S FLAP OPERATION:
• It is posteriorly based flap which gets its supply from the greater palatine artery.
• Local anesthesia is infiltrated on the palatal aspect. Infilteration is also given on the buccal side of the oroantral defect.
• Removal of fistula tract and clearing any signs pathology.
• The flap is outlined with surgical marking an excess of what appears to be required to rotate the flap.
• Incision is placed to the bone making sure the palatal pedicle is kept intact.
• A full thickness mucoperiosteal flap is reflected with care taken to visualize the greater palatine vessels.
• A small amount of tissue along the margin of the defect on the buccal aspect is also reflected to enable suturing.
• The flap is reflected and rotated to fit the defect. There are chances of ending of the tissue when it is turned to cover the oroantral opening.
• The flap is sutured to the buccal flap ensuring a good water tight seal.
• The raw surface of the palate is left to granulate only.
• A small gauze soaked in Whitehead’s varnish may be placed on that raw surface for a few days.

REFERENCES:
- Textbook of Oral & Maxillofacial Surgery, Chitra Chakravarthy (2nd Edition)
- Slideshare
- researchgate.net

