• Also known as PARTSCH II or CYSTECTOMY.
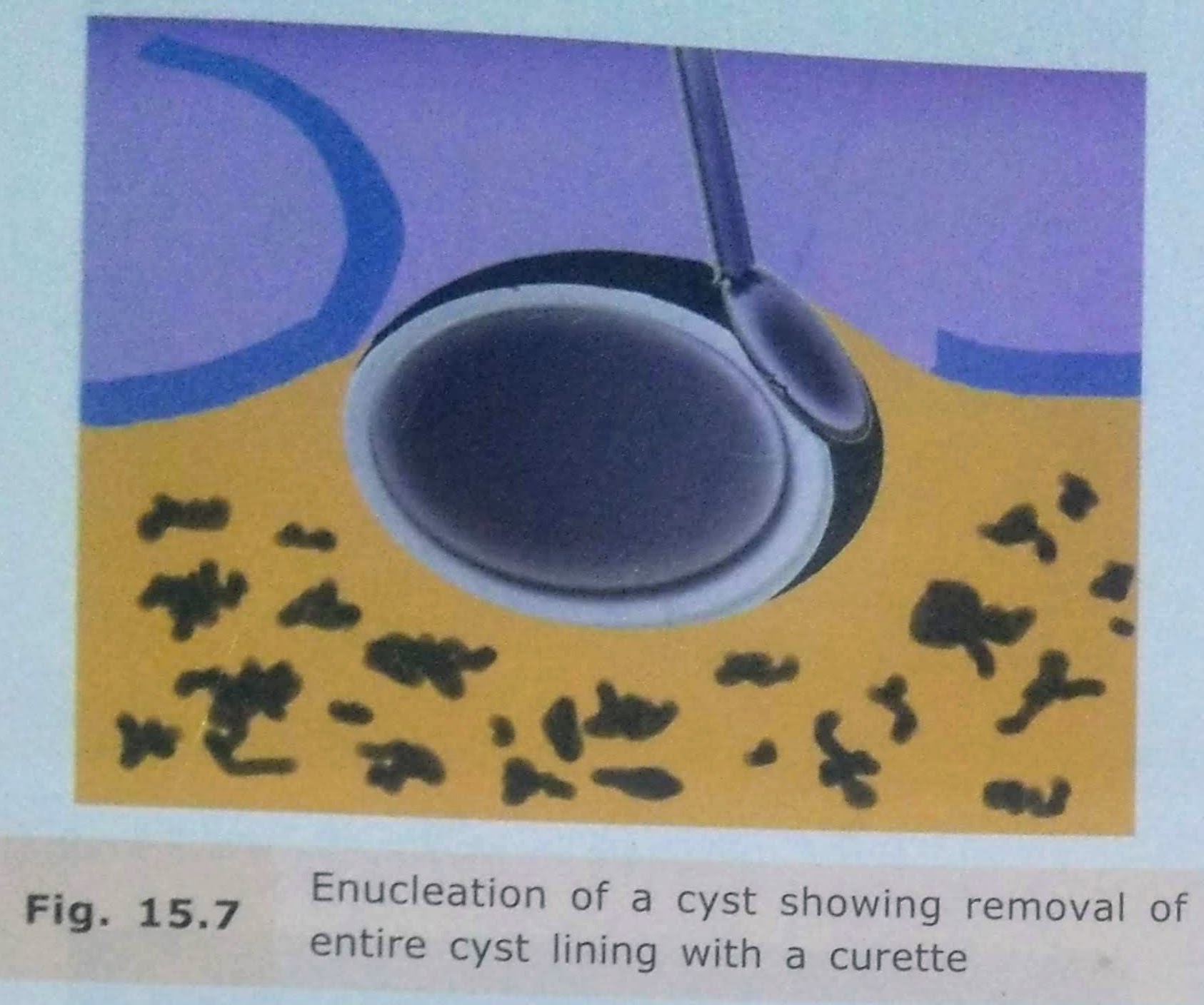
• Enucleation is the surgical removal of the entire cystic lining in to-to.
By definition, it means shelling out of the entire cystic lining without rupture.
This surgical procedure leaves behind a hollow cavity in bone covered by oral mucoperiosteum.
This gets filled up with blood clot which eventually organizes to form healthy bone.
INDICATIONS:
• Is the treatment of choice for removal of cysts of jaws+ should be employed with any cyst of the jaw, that can be safely removed without sacrificing underlying structure.
ADVANTAGES:
- Entire pathological tissue is removed from the lesion.
- Tissue available for histopathological examination
- Chances of recurrence are less.
- Healing time is faster and less appointments for the patient.
- Enucleation with primary closure eliminates the repeated appointments for packing medicated gauze irrigation & fabrication of plug.
DISADVANTAGES:
1.Relatively radical procedure.
2.Chances of devitalising the adjacent teeth.
3.Chances of fracture of the jaw.
4.Risk of creation of oroantral/oronasal communication
TECHNIQUES:
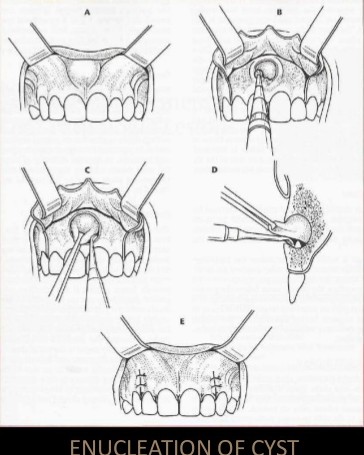
Enucleation with Primary Closure:
• Small cysts can be removed under local anaesthesia
• large cyst should be taken out under general anesthesia, as they are close to vital structures and blood vessels.
• After achieving adequate anesthesia, a mucoperiosteal incision is made such that the incision rests on sound bone.
• Mucoperiosteal flap is reflected taking care not to perforate rate the cystic lining.
• If the bone is perforated by the cyst, the lining will be adherent to the periosteum and will be difficult to reflect it.
• The cystic lining is exposed and now carefully teased away from the bone.
• It is relatively easy to separate the cystic lining from the bone because there is a layer of fibrous tissue between the two which is easily separabl.
• In case of infected cysts or an odontogenic keratocyst. the cystic lining is friable and more difficult to remove entirely.
• Every attempt is made to remove the entire cystic lining in a single piece without perforating it.
• This ensures complete removal.
• After the cyst is removed completely, the cavity in irrigated thoroughly, hemostasis ensured, sharp bone debris are filed and the flap replaced and sutured.
Enucleation with Open Packing :
• In case of a large cyst which was previously infected closure may not be possible
• After enucleation, the wound is then packed with me impregnated with bismuth iodoform paraffin paste (BIPP) or Whitehead’s varnish.
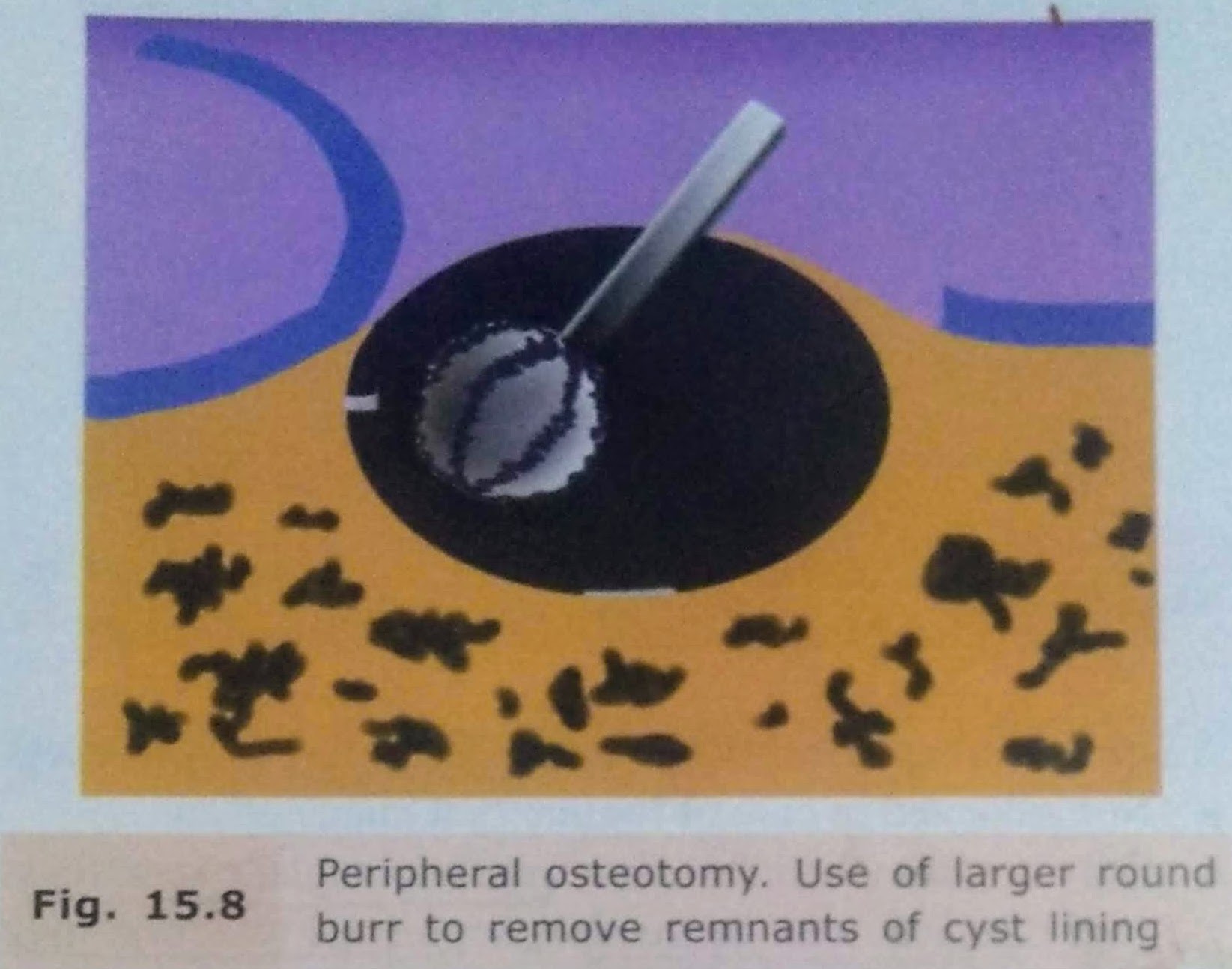
Enucleation with Peripheral Osteotomy:
- In this procedure, instead of using a curette, a large round bur may be used to remove around 1-2 mm of bone around the entire periphery of the cystic cavity.
- This is done to ensure that any remaining epithelial cells present in the cystic wall or bony cavity are removed.
Enucleation with Bone Curettage:
• After enucleation, if there is a doubt that a part of the line has been left behind, it can be curette out.
• A bone curette is used to scrape the band remove any remaining lining
Enucleation with Peripheral Osteotomy
• In this procedure, instead of using a curette, a large round bur may be used to remove around 1-2 mm of bone around the entire periphery of the cystic cavity.
• This is done to ensure that any remaining epithelial cells present in the east wall or body cavity are removed.
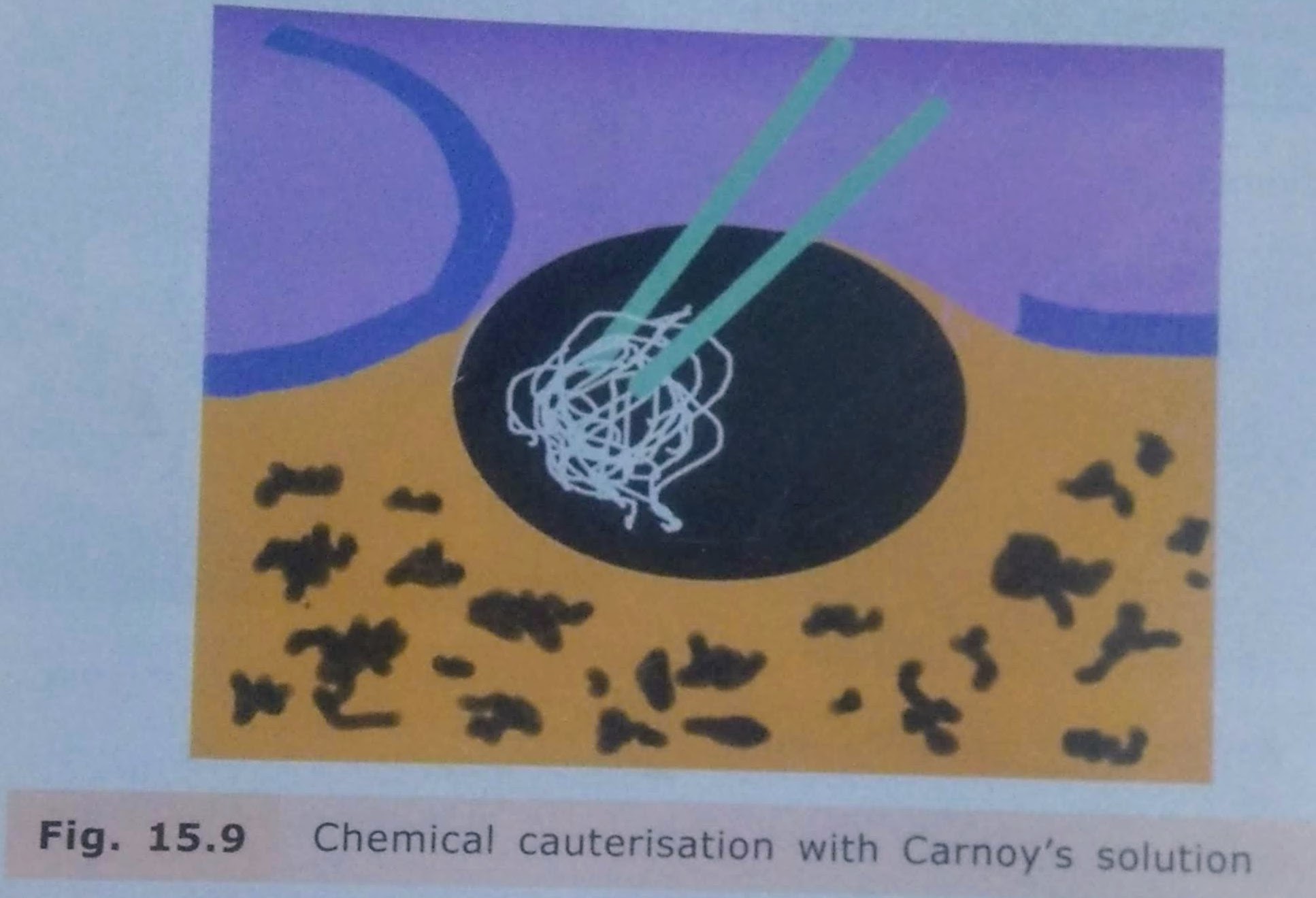
Enucleation with Chemical Cauterisation:
• It is indicated mainly in cases of odontogenic keratocyst.
• After enucleation, to remove any remaining lining of the cyst chemical cauterising agent Carnoy’s solution is applied along the walls of the cystic cavity.
• It is left for about 5-7 minutes and then irrigated thoroughly with saline.
• This solution chemically cauterizes any remaining cells of the system.
Enucleation with Bone Grafting
• Bone grafting with autogenous cancellous bone grafts can be done in case of large bony defects.
• The bone graft obliterates the cavity and stimulates osteogenesis.
• There is, however, a risk of wound breakdown and infection of the bone graft which may lead to failure.

COMPLICATIONS:
• Risk of bone fracture due to cyst.
• Inferior dental nerve involvement.
• Management of teeth related to cyst.
• Oroantral Communication.
• Hematoma formation.
• Infection.
• Dead Space: At surgical procedure, a hollow dead space is formed. It is usually filled up with blood clot and eventual bone formation.
However, there are chances of infection of the clot, breakdown of suture line and pus discharge.
REFERENCES:
• Textbook of Oral & Maxillofacial Surgery, Chitra Chakravarthy (2nd Edition)
• SlideShare

