• The mitral valve apparatus is a funnel-shaped structure with its apex beat on the left ventricle.
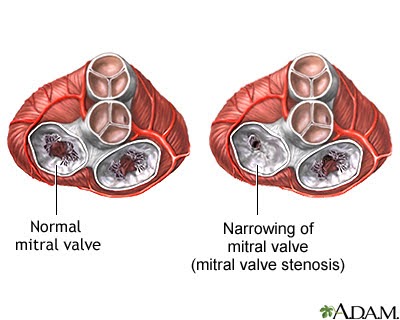
• Mitral Stenosis is the narrowing of the mitral valve of the heart.
• Leads to complications due to the impairment of blood flow
• More commonly seen in females.
• Most Common cause : Rheumatic Heart Disease.

ALTERED ANATOMY IN RHEUMATIC MITRAL STENOSIS
- Primary Pathologic Features:
• Thickened mitral cusps with/without calcification.
• Fusion of valve commissures.
• Shortening & fusion of chordae tendineae. - Secondary Pathological Features:
• Left atrial hypertrophy & dilatation.
• Left atrial thrombi.
• Changes in venous & arterial hypertension in pulmonary vasculature.
ETIOLOGY:
• Rheumatic fever.
• Congenital mitral Stenosis
• Systemic Lupus Erythematosus (SLE)
• Malignant carcinoid
• Gout
• Atrial Myxoma
• Infective Endocarditis (rare)
• Rheumatoid Arthritis (rare)
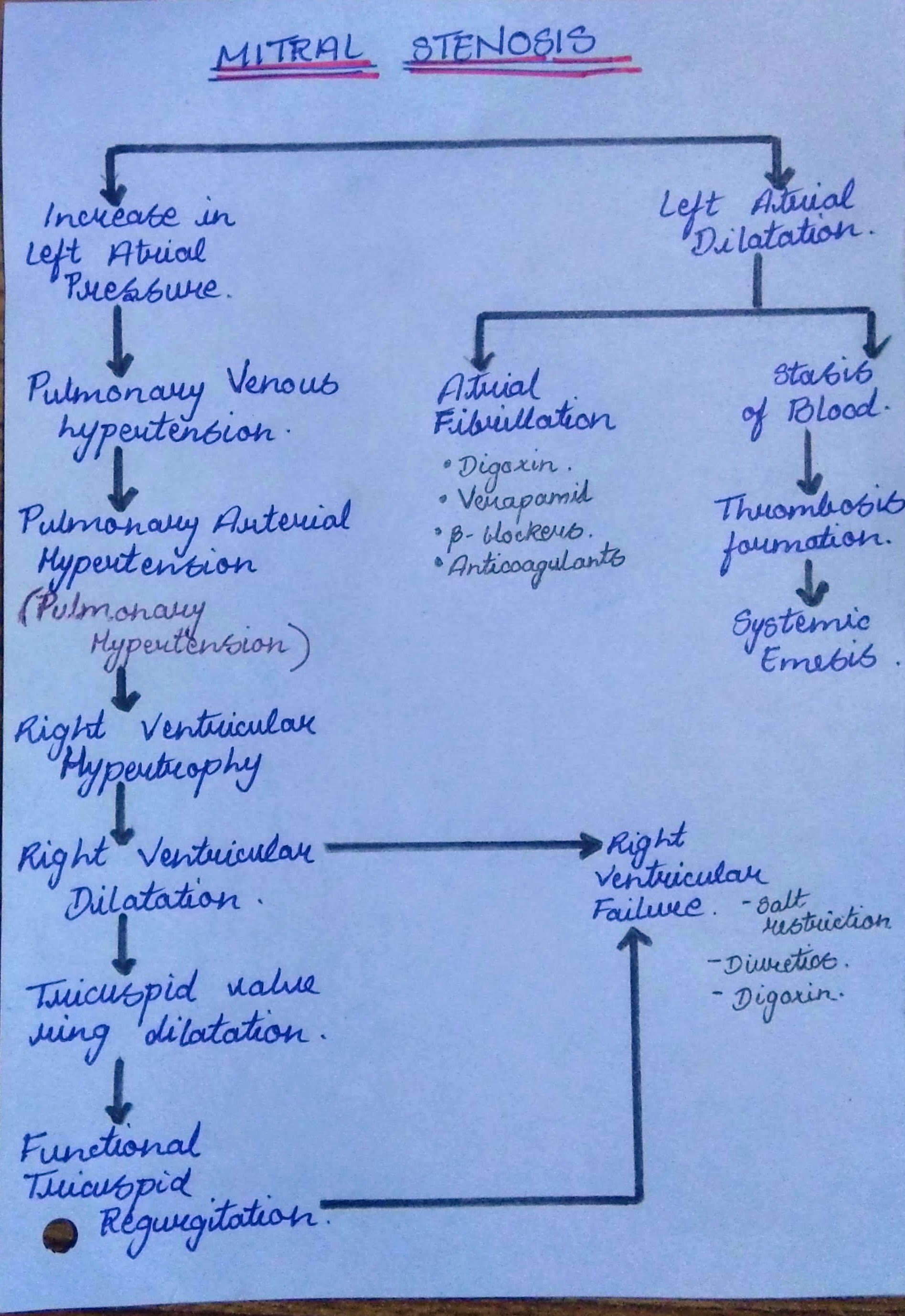
PATHOPHYSIOLOGY:
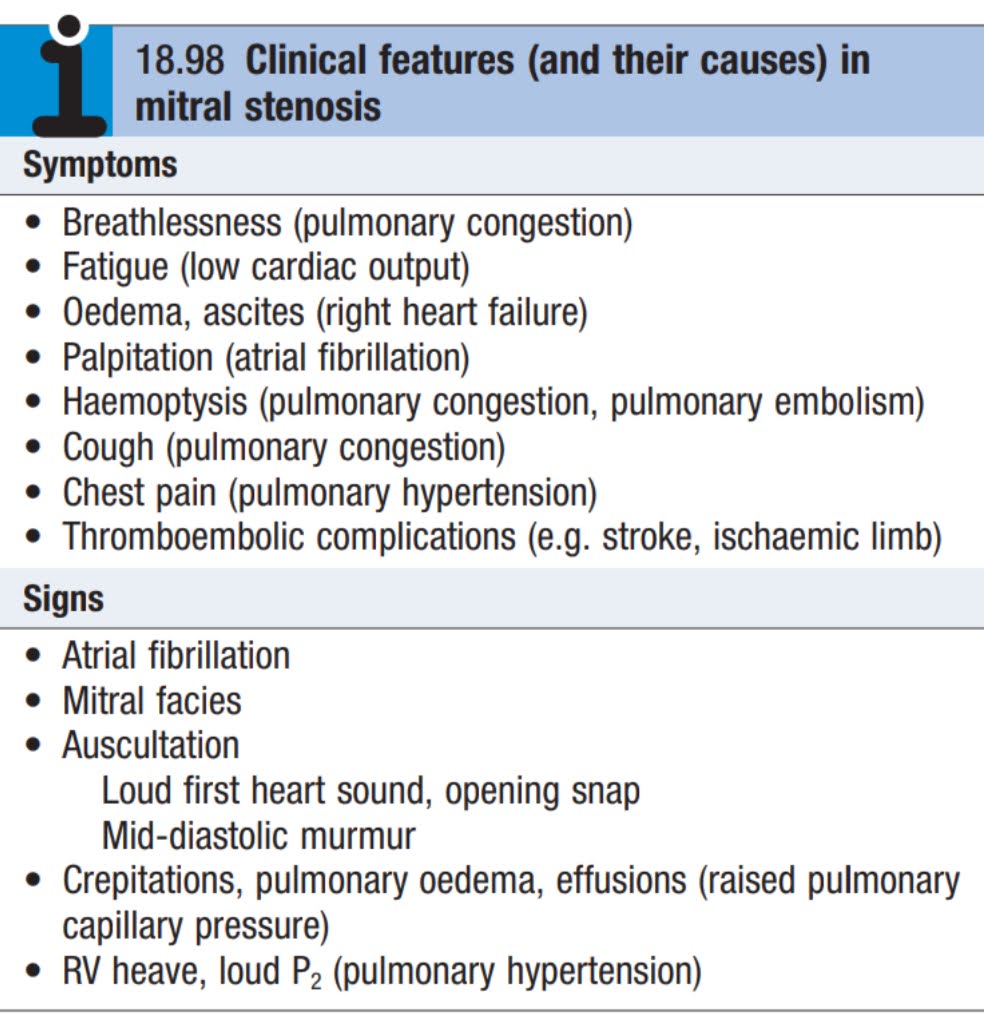
CLINICAL FEATURES:
• Early presentation of Mitral stenosis include breathlessness on exertion and fatigue.
• As stenosis progresses, patients are dyspnic on rest.
• They have orthopnoea & paroxysmal nocturnal dyspnoea.
• Acute pulmonary oedema may occur.
• Haemoptysis: due to rupture of pulmonary-bronchial connection.
• Edema of lower limbs.
• Thromoembolic events like stroke, limb ischaemia
• Winter bronchitis: Patient with myocardial infarction are prone to recurrent attacks of bronchitis, particularly during winters.
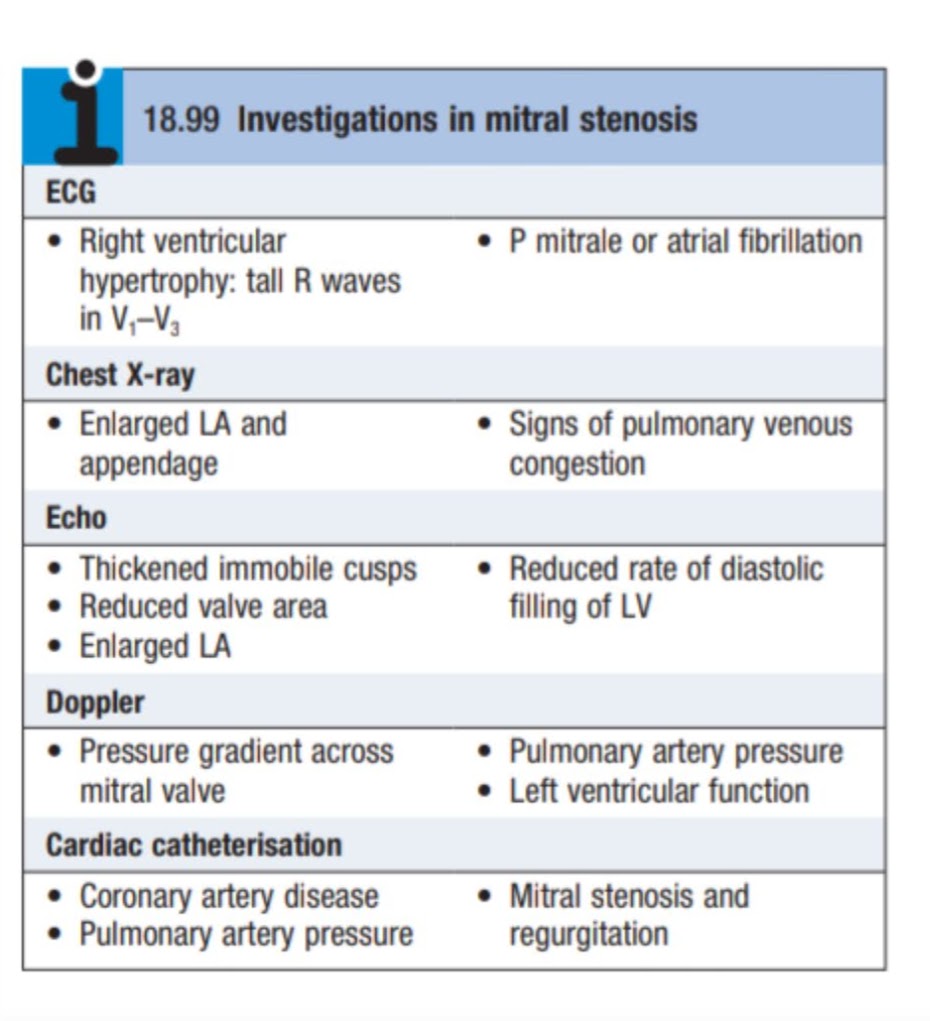
INVESTIGATIONS:
• ECG: May indicate left atrial(LA) enlargement, right ventricular hypertrophy and atrial fibrillation.
• CHEST X-RAY: LA enlargement, pulmonary congestion.
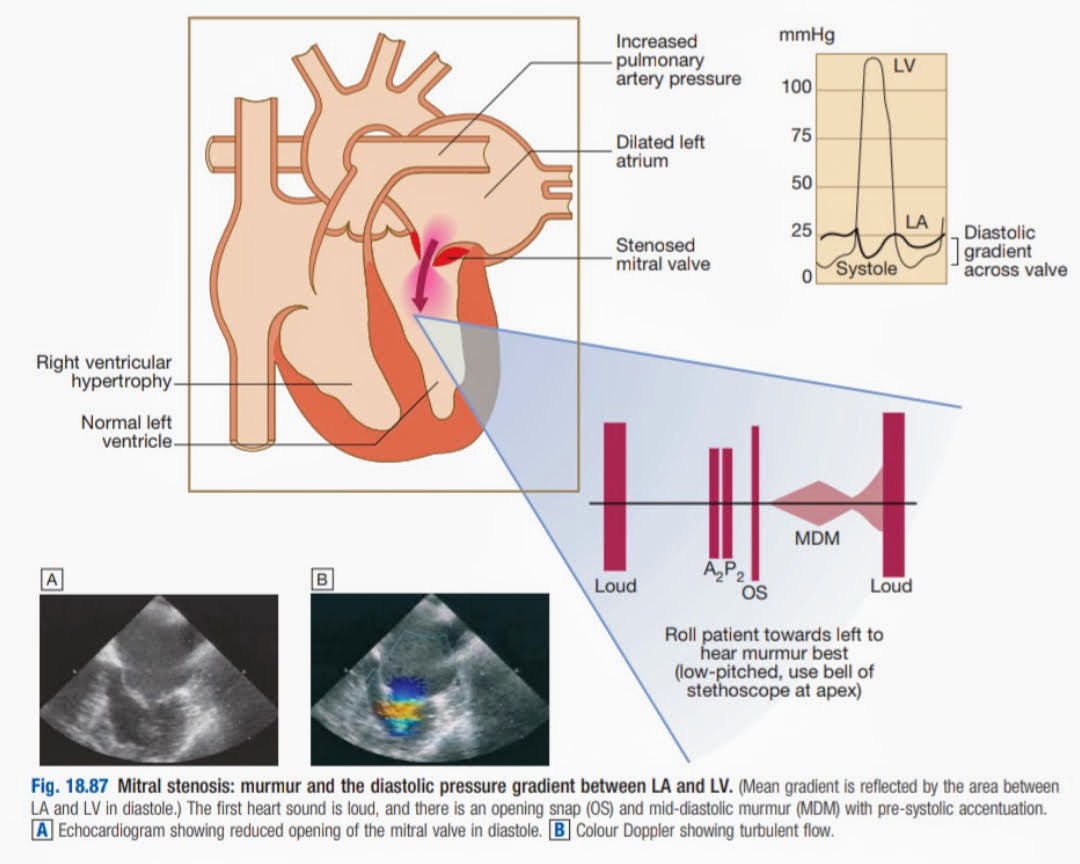
• ECHOCARDIOGRAPHY: Most sensitive & specific non-invasive methods to diagnose valvular disease.
- May reveal structural abnormalities of the valve.
- Size of cardiac chambers.
- Pulmonary artery pressure.
- Ventricular dysfunction & presence of thrombi.
CARDIAC CATHETERIZATION: Used to assess associated valvular lesions & to detect coronary artery disease.
MANAGEMENT:
- Treatment of atrial afibrillation
-Anticoagulants. – Verapamil. -Digoxin. – Beta blockers.
2. Treatment right ventricular failure:
- Salt restrictions.
- Diuretics
- Digoxin.
3. Restriction of physical activity.
4. Prophylaxis should be given to all patients to prevent rheumatic fever.
5. Prophylaxis for Infective Endocarditis should be given prior to the procedure.
SURGICAL MANAGEMENT:
- MITRAL VALVECTOMY
Percutaneous Balloon Valvotomy:
- Indicated when mitral valve is non-calcified &without regurgitation.
- Procedure involves passing of a catheter across the valve & inflation of the balloon to dilate the orifice.
Open Valvotomy:
- Carried out in patients where balloon valvotomy is not possible or in cases with restenosis(*means that a section of blocked artery that was opened up with angioplasty or a stent has become narrowed again)
- In this procedure, the fusion of the valve is loosened, Ca(calcium) deposits and thrombi are removed.
2. MITRAL VALVE REPLACEMENT:
o Mitral Valve is replaced when there is critical mitral stenosis(<1cm² of orifice size)
o And/or there is an associated significant mitral regurgitation.
o Replacement done,when mitral valve is severely distorted & calcified.
COMPLICATIONS:
o Atrial fibrillation
o Pulmonary Hypertension
o Right Ventricular Failure
o Systemic thromboembolism
o Winter Bronchitis
o Ortner’s Syndrome
REFERENCES:
- Davidson’s Principle and Practise of Medicine
- Medicine Prep Manual for Undergraduate, K George Mathew(4th Edition)
- Mayoclinic.org
- Medlineplus.gov
- Medmovie.com

