🔹EXAMINATION:
A. Inspection & Palpation:
Normal ⬇️
- Bilaterally Symmetrical
- Ellipsoidal in shape
- Transverse diameter > Antero-posterior diameter
- Acute subcostal angle
▪️Abnormal shapes of chest:
1) Pigeon Breast/Keeled chest – Rickets

- Ricketic Rosary – cartilagenous overgrowth at costochondral junction.
- Harrison sulcus – indrawing of soft ribs during inspiration.
2) Funnel Chest/Cobbler’s chest –
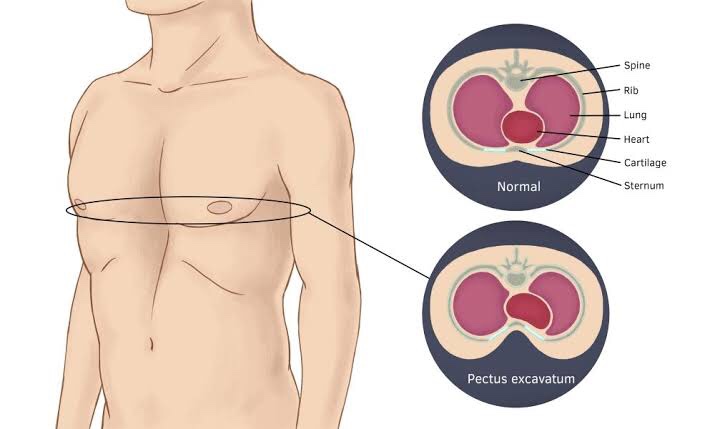
Image©️healthand.com

3) Barrel shaped chest – Emphysema
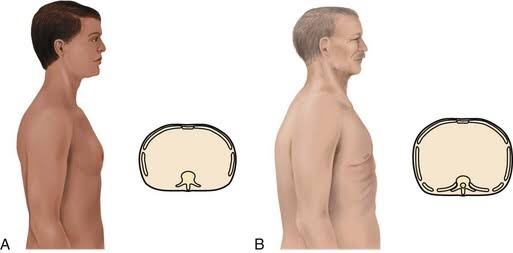
- Increased A-P diameter, wide subcostal angle
- Sternum more arched
- Spine – concave
- Ribs – less oblique
4) Spinal Deformities – Scoliosis

Alar Chest – In advanced TB, scapula is winged
▪️Respiratory Rate:
Range: 16 – 20 beats/min.

▪️Respiratory Rhythm:
1) Cheyne-Stokes Respiration:
➡️ Alteration of apnea & hyperpnea due to anoxemia. Therefore CO2 accumulation in body causing hyperventilation.
➡️ Causes:
- Left ventricular failure(LVF)
- ⬆️ Intracranial pressure(ICP)
- Poisoning
- Uremia
- Deep sleep
2) Kausmaul’s Breathing:
- Air hunger(Rapid & Deep)
- Diabetic Ketoacidosis, alcoholic, starvation, uremia
3) Bitot’s Respiration: Meningitis
▪️Type of breathing:
- Abdominothoracic – males
- Thoracoabdominal – females
- Thoracic – Severe Ascitis
- Abdominal – Collapse of lung
▪️Movements:
Unilateral diminished movement–
- Pleural effusion
- Consolidation
- Fibrosis
Bilateral movement–
- Bronchial Asthma
- Emphysema
▪️Mediastinum:
➡️ Shift detected by noting position of Trachea (suprasternal notch) / Apex beat (5th Inter-costal space)
➡️ Trail’s sign: It is the undue prominence of the clavicular head of sternomastoid on the side to which the trachea is deviated.
▪️Vocal Fremitus:
➡️ Tactile perception of viberations to chest wall from larynx during act of phonation.
- Increased – consolidation
- Decreased – Pleural effusion, pneumothorax, Asthma, fibrosis, collapse, emphysema
B. Percussion:
➡️ Normal: Resonant
- Impaired – ⬇️ air in lungs
- Dull, stony dull note (effusion)
- Tympany (emphysema, pneumothorax)
➡️ Normal liver dullness –
The “5-7-9 rule”
- The upper border of liver dullness is defined by:
- 5th intercostal space in the midclavicular line
- 7th intercostal space in the midaxillary line
- 9th intercostal space in the scapular line

➡️ If present in 4th space – Amoebic abscess of liver
➡️ If present in 6th space –
- Pneumonia
- Cirrhosis (Terminal)
- Air in peritoneal cavity
➡️ Pneumothorax – shifting dullness (both air + fluid)
C. Auscultation:
Image©️pinterest
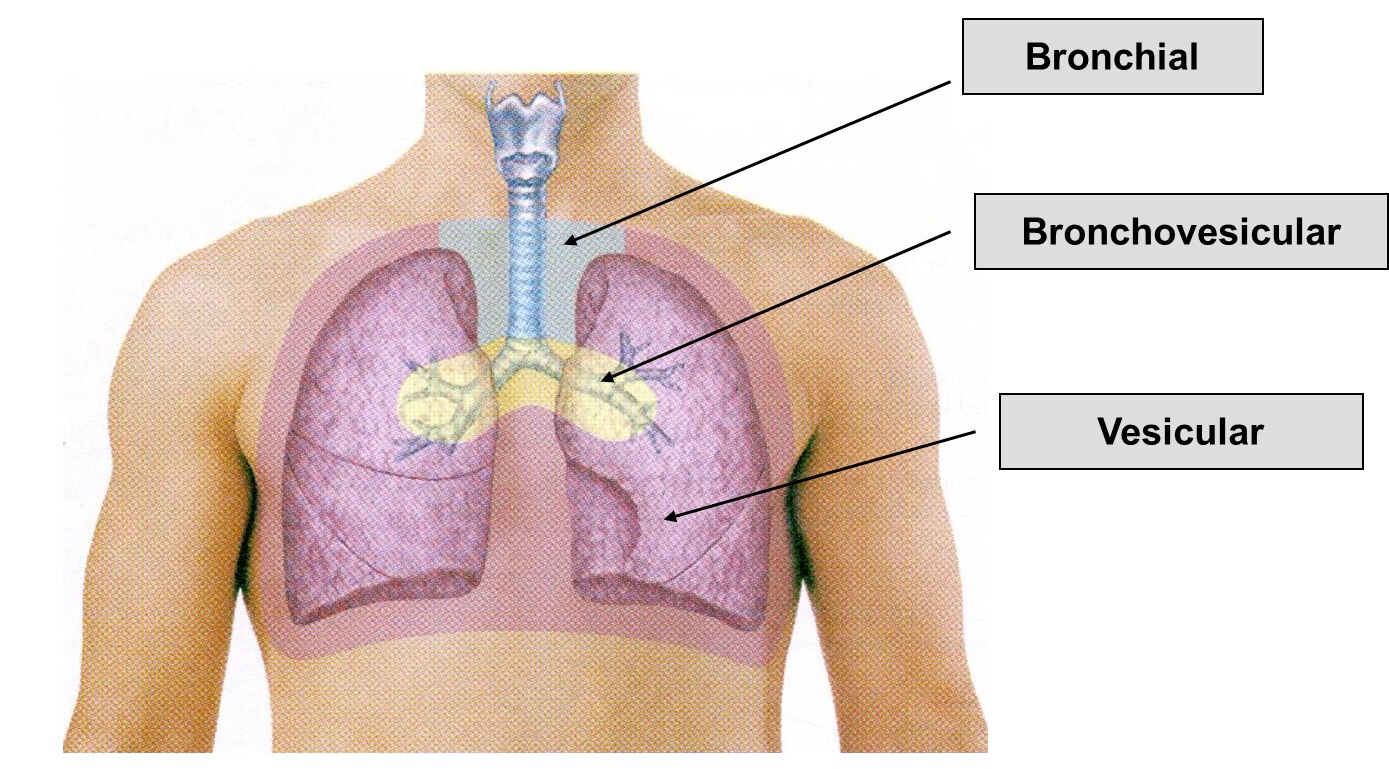
1) Vesicular breath sounds:
➡️ Vesicular breath sounds are heard across the lung surface. They are lower-pitched, rustling sounds with higher intensity during inspiration. During expiration, sound intensity can quickly fade. Inspiration is normally 2-3 times the length of expiration.
➡️ Various Types of Vesicular Breath Sound:
- Exaggerated or puerile vesicular breath sounds: It is normal vescicular breathing with relatively greater clarity. It is common in children and thin built individual.
- Diminished or absent breath sounds: Various causes are shallow breathing, airway obstruction, bulla, hyperinflation, pneumothorax, pleural effusion or thickening, and obesity.
- Normal vesicular breath sound with prolonged expiration: It can occur in obstructive airway diseases like asthma and chronic bronchitis.
2) Bronchial breath sounds:
➡️ The bronchial breath sounds over the trachea has a higher pitch, louder, Expiratory phase is longer than inspiratory phase and there is a pause between inspiration and expiration.
➡️ It is normally heard anteriorly over the manubrium and posteriorly between the C7 and T3 vertebrae.
➡️ The vesicular breathing is heard over the thorax, lower pitched and softer than bronchial breathing.
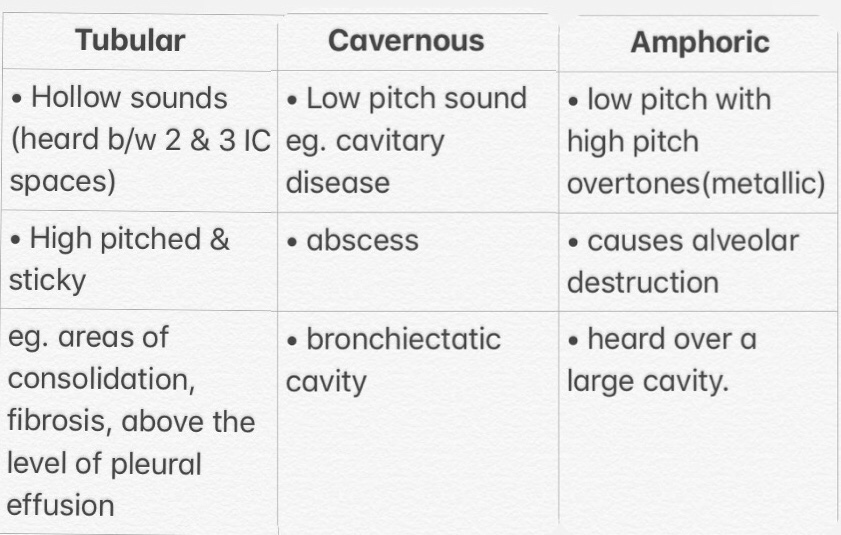
Bronchial sound types👇🏻
3) Bronchovesicular breath sounds:
➡️ It is intermediate between bronchial and vescicular breathing. It has intermediate intensity and pitch with same duration of inspiratory and expiratory phase. It is normally heard anteriorly over 1st and 2nd intercostal spaces and between scapulae posteriorly.
▪️Foreign Sounds:

References:
- https://stanfordmedicine25.stanford.edu/the25/pulmonary.html
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4518345/
- http://www.oxfordmedicaleducation.com/clinical-examinations/respiratory-examination/breath-sounds/

