7) TUBERCULOSIS (TB)
▪️ Causes: Health Care Workers, Poverty, Overcrowding, Diabetes Mellitus, Silicosis, Alcohol, Immuno-compromised states.
▪️Presentation:
- Low grade fever with evening rise.
- Cough
- Malaise
- Loss of Weight
- Night sweats
- Haemoptysis
▪️Treatment:
- Active TB
- 4-drug regimen of rifampin, isoniazid, pyrazinamide and ethambutol (2 months)
- continuation of rifampin and isoniazid (4 months)
- latent TB
- rifampin and isoniazid (3 months)
- OR isoniazid alone (6 months)
- consideration of multidrug-resistant TB
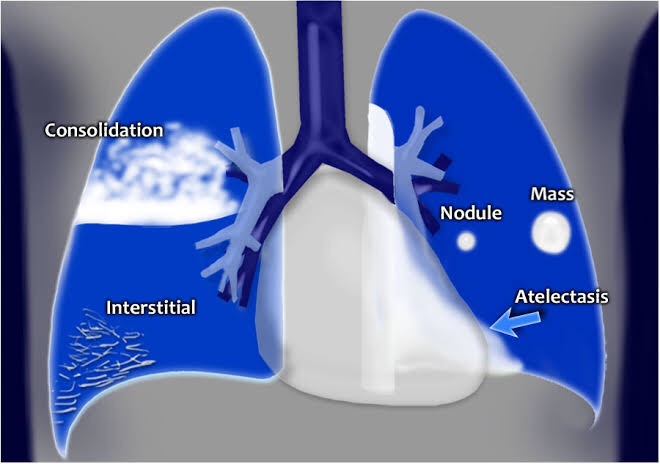
▪️Radiological forms:
- Fibrosis/Cavity – Post primary infection (Refer page 3)
- Consolidation – Primary infection (parenchymal): Refer page 5
- Collapse (Refer page 4)
- Tuberculous Pleural Effusion (Refer page 2)
- Miliary Tuberculosis –
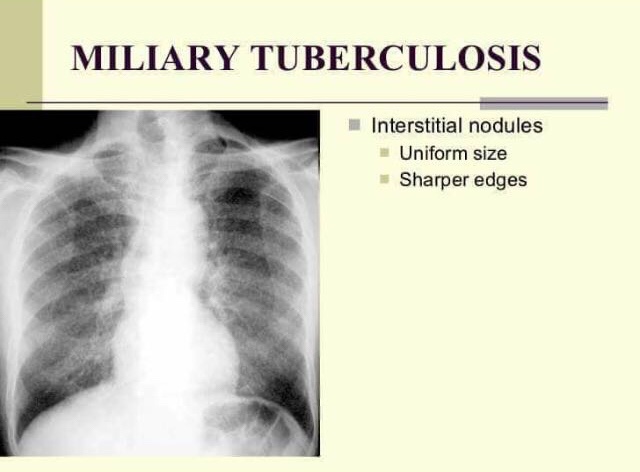
• uniform size and distribution throughout both lungs
Page 7 of 14
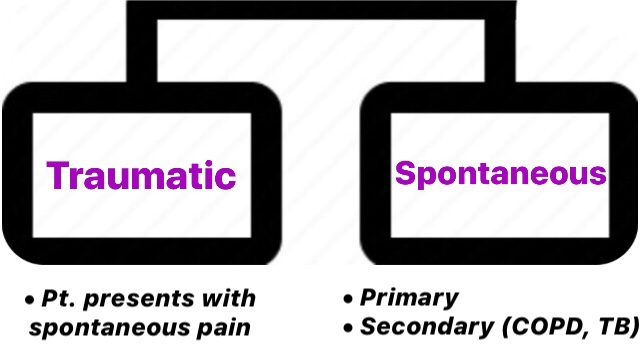
8) PNEUMOTHORAX
➡️ Pneumothoraces are collections of gas within the pleural space. If the pneumothorax is under pressure, it is called a tension pneumothorax.
Pneumothorax

Chest radiograph (Right sided Pneumothorax)
The three main features of a pneumothorax on a chest x-ray are:
- peripheral translucency
- Definite lung edge
- the absence of lung markings peripheral to lung edge
- Mediastinal shift to the opposite side
▪️Treatment:
- small pneumothorax with minimal symptoms
- primary spontaneous pneumothorax: discharge with early outpatient follow-up and advised to return if symptomatic
- secondary pneumothorax: observe with high-flow oxygen therapy and consider intervention
Page 8 of 14

