🔹 Introduction:
➡️ They are clearly visible & can be easily diagnosed as per the clinical features alone – high viral load. They are useful markers of disease progression & immuno-suppression.
➡️ The EC (1995) gave two diagnostic criterias:
- Presumptive (initial clinical appearance)
- Definitive (special investigation for diagnosis)
🔹 Classification:
1) Group 1 lesions: (Lesions strongly associated with HIV infection)
🔸 Candidiasis – 4 clinical patterns observed
- Pseudomembranous
- Erythematous
- Hyperplastic
- Angular cheilitis
🔸 Hairy Leukoplakia – Associated with EBV
- Lateral borders of tongue as painless, faint white vertical streaks or thickened & furrowed areas with shaggy keratotic surface – imparting corrugated appearance.
- Homosexual males
- Basal epithelial cells – harbour EBV (Latent)
⬇️
Langerhan cells by HIV
⬇️
cause reactivation of EBV
⬇️
epithelial hyperplasia
- Histological Features:
- Acanthosis, hyperkeratosis
- Balloon cells – upper prickle layer
- Epithelial cells show Nuclear beading
🔸 Kaposis’s Sarcoma (HHV-8)
🔸 Non-hodgkin’s lymphoma
🔸 Periodontal Disease
- Linear Gingival Erythema
- NUG
- NUP
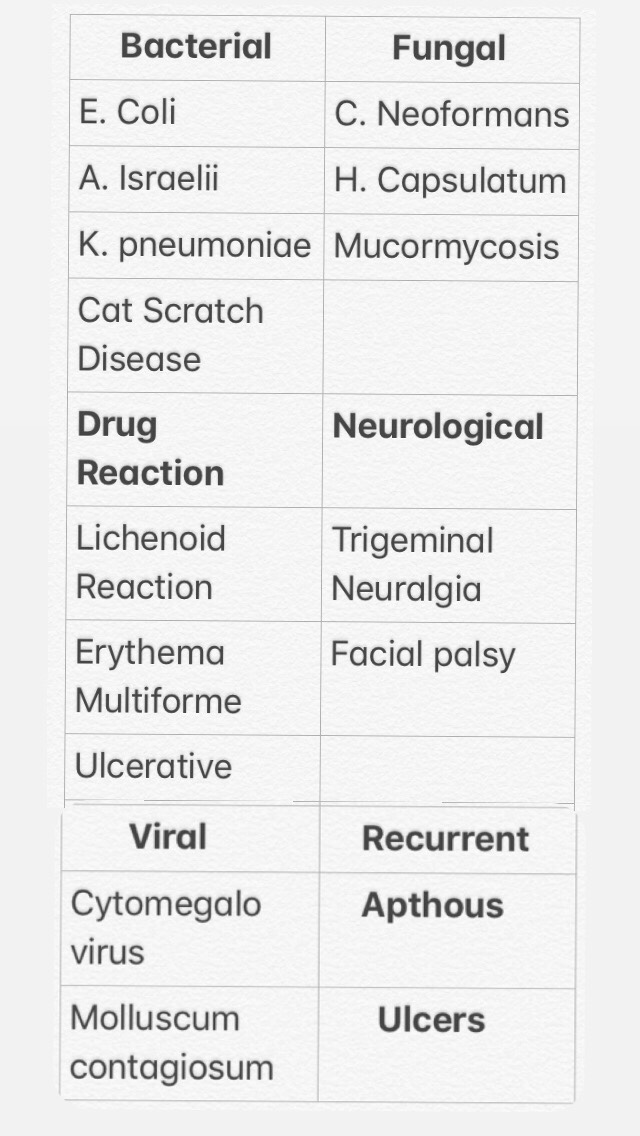
2) Group 2 Lesions: (Less Common)
🔸 Bacterial infection
- Mycobacterium TB
- Mycobacterium avium
🔸 HSV, Herpes Zoster
🔸 Melanotic hyperpigmentation (Brown-black intra-oral focal/diffuse Macules)
🔸 Necrotizing Ulcerative Stomatitis
3) Group 3: (Lesions associated with HIV infection)
Dr. Mehnaz Memon🖊
References: Ghom’s Oral medicine & Internet

