The thyroid gland is found at the base of your neck and lies just below your Adam’s apple. This gland produces hormones that are important to your metabolism, known as T3 and T4.
- Some T3 is secreted by the thyroid, but most is produced by deiodination of T4 in peripheral tissues.
- Both T4 and T3 are bound to carrier proteins (thyroid-binding globulin [TBG], transthyretin [binds T4], and albumin) in the circulation.
- Increased levels of total T4 and T3 with normal free levels are seen in states of increased carrier proteins (pregnancy, estrogens, cirrhosis, hepatitis, and inherited disorders).
- Conversely, decreased total T4 and T3 levels with normal free levels are seen in severe systemic illness, chronic liver disease, and nephrosis.
Since we know that the thyroid hormones play an important role in regulating your body’s metabolism, it makes sense that a decrease in these hormones would lead to symptoms such as a loss of energy, an increased need for sleep, an intolerance to cold, a slow pulse, constipation, weight gain, and depression
causes
- Autoimmune hypothyroidism: Hashimoto’s thyroiditis, atrophic thyroiditis
- Subtotal or total thyroidectomy
- Neck radiation in cancer patients suffering with Hodgkins lymphoma and laryngeal cancer
- Drugs: iodine excess, lithium and antithyroid drugs
- Congenital hypothyroidism
- Iodine deficiency
- Infiltrative disorders: amyloidosis and sarcoidosis
- Transient – Postpartum thyroiditis and Subacute thyroiditis
- Withdrawal of thyroxine treatment
- Secondary- Hypopituitarism and Hypothalamic disease, tumors, trauma, infiltrative disorders, idiopathic
Clinical Features
- lethargy/ fatigue
- mild weight gain with poor appetite
- constipation
- cold intolerance
- cool peripheral extremities.
- menorrhagia
- dry skin and hair loss,
- difficulty concentrating and poor memory
- Cardinal features on examination include
– bradycardia,
– mild diastolic hypertension - prolongation of the relaxation phase of deep tendon reflexes
- Goiter may be palpated, or the thyroid may be atrophic and nonpalpable.
EVALUATION OF HYPOTHYROIDISM
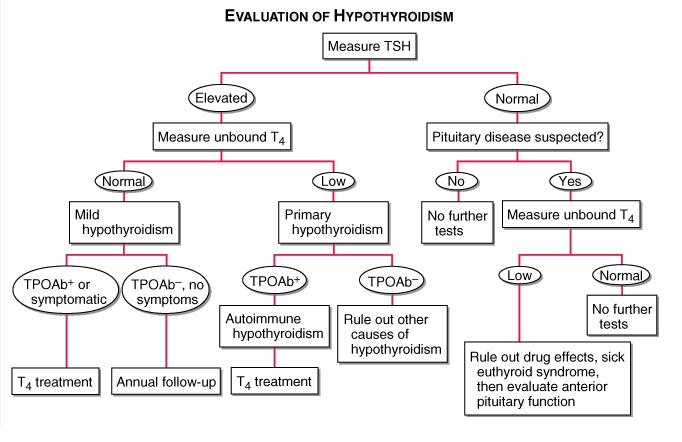
- TPOAb+, thyroid peroxidase antibodies present; TPOAb–, thyroid peroxidase antibodies not present;
- Decreased serum free T4 is common to all varieties of hypothyroidism.
- An elevated serum TSH is a sensitive marker of primary hypothyroidism but is not found in secondary hypothyroidism.
- Elevated cholesterol
- Increased creatine phosphokinase
- Anemia may be present
- Bradycardia, low-amplitude QRS complexes, and flattened or inverted T waves may be present on ECG.
Treatment
- Adult pts <60 years without evidence of heart disease may be started on 50–100 μg of levothyroxine (T4) daily.
- In the elderly or in pts with known coronary artery disease, the starting dose of levothyroxine is 12.5–25 μg/d.
- In secondary hypothyroidism, TSH levels cannot be used, and therapy needs to be guided by free T4 measurement.
- Women on levothyroxine replacement should have a TSH level checked as soon as pregnancy is diagnosed, as the replacement dose typically increases by 30–50% during pregnancy. Failure to recognize and treat maternal hypothyroidism may adversely affect fetal neural development.
- Therapy for myxedema coma should include levothyroxine (500 μg) as a single IV bolus followed by daily treatment with levothyroxine (50–100 μg/d), along with hydrocortisone (50 mg every 6 h) for impaired adrenal reserve, ventilatory support, space blankets, and treat- ment of precipitating factors.

